![]()
Last updated: April 2026 · For adults 19+ in Canada · Informational only · Not medical advice
Psilocybin and SSRIs/SNRIs: What People Report vs What Studies Suggest
Medical disclaimer: This article is for general education only. It is not medical advice. It is not telling you to start, stop, or change any medication or drug. Changing antidepressants can be risky (withdrawal, relapse). Talk to your prescribing doctor about your own situation.
Quick summary: Many people on SSRIs or SNRIs say psilocybin feels weaker. Big surveys and some lab studies back that up. No one can promise what will happen to you. Do not raise your dose to “make up” for blunting – that can be dangerous.
If you want to know how psilocybin (the active ingredient in magic mushrooms) might interact with SSRIs and SNRIs, you are not alone. Forums are full of personal stories. Researchers run surveys and clinical trials. Both are useful, but they answer different questions.
This article compares what people say online with what a few strong studies measured. For more background on mood and mushrooms, see Shroom Bros on magic mushrooms and depression, mental health and mushrooms, and what psilocybin therapy is.
What are SSRIs and SNRIs? (Simple version)
SSRIs stand for selective serotonin reuptake inhibitors. Common examples include sertraline (Zoloft), escitalopram (Lexapro), and fluoxetine (Prozac). They mostly work by helping the brain keep more serotonin available. Doctors often prescribe them for depression and anxiety.
SNRIs are serotonin-norepinephrine reuptake inhibitors. Examples include venlafaxine (Effexor) and duloxetine (Cymbalta). They affect serotonin and another chemical called norepinephrine.
Trusted overviews: NIMH on mental health medications and MedlinePlus on antidepressants.
What is psilocybin doing in the brain? (Still simple)
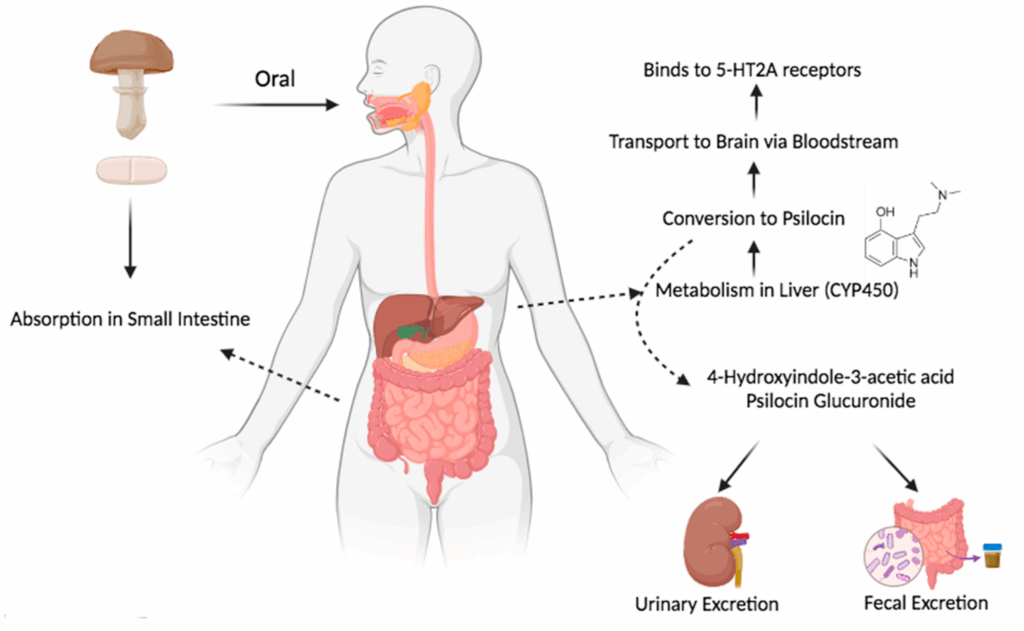
Psilocybin turns into psilocin in the body. Psilocin attaches to certain serotonin receptors, especially 5-HT2A. That receptor is part of why people see shifts in perception, mood, and thinking during a trip. For a longer read on brain change after mushrooms, see psilocybin and neuroplasticity.
Because antidepressants also touch the serotonin system (in a different way than psilocin), scientists always wondered if mixing the two could dull or change a trip.
Why research studies often ask people to stop antidepressants first
In many psilocybin therapy trials, people are asked to taper off serotonergic antidepressants and wait a washout period before a study dose. Reasons include safety, clearer results, and older data suggesting meds can blunt psychedelic effects.
Big-name trial papers you can open yourself: Davis et al., 2021 (JAMA Psychiatry) and Carhart-Harris et al., 2021 (New England Journal of Medicine).
Important: What a study protocol allows is not the same as what is safe for random home use. Trials have doctors, fixed doses, and rules. Real life has mixed drugs, unknown mushroom strength, alcohol or cannabis on the side, and no nurse in the room.
What people say online (patterns, not proof)
Reddit threads are not a random sample. People with wild stories post more than people with boring nights. Still, the same lines show up a lot. Think of these as themes, not facts.
- “My trip felt weaker on my SSRI.” Often same product and dose as before, but less intensity or shorter peak.
- “I stopped my SSRI for a week and it still felt weak.” People argue about how long blunting lasts.
- “I tripped hard on an SNRI anyway.” Bodies differ. Dose, genetics, liver health, batch strength, and setting all matter.
- “Will I get serotonin syndrome?” Some threads panic. Others say “never happens.” The truth is calmer and more careful than both (see below).
- Microdosing while medicated. Stories are mixed. For basics on microdosing (not drug interaction advice), read microdosing 101 and what is microdosing.
Compared with studies, online posts usually lack hard details: no blood levels, no lab-tested mushroom dose, no list of other drugs taken that night.
Study 1: Gukasyan et al., 2023 (big survey after the fact)
Researchers ran a large online survey of people who had used psilocybin mushrooms while on an antidepressant and/or within two years after stopping one. Full paper: DOI 10.1177/02698811231179910 (Journal of Psychopharmacology).
While still on medication
There were 611 reports of using mushrooms while on an antidepressant. People compared how strong the trip felt versus what they expected. Rough odds of weaker than expected effects:
- About 47% (SSRIs) – think “nearly half”
- About 55% (SNRIs) – a bit higher than SSRIs in this survey
- About 29% (bupropion) – bupropion is a different kind of antidepressant, not a classic SSRI/SNRI
So: weaker trips on meds are common in this data set. That does not mean everyone feels nothing.
After stopping medication
There were 1,542 reports after people stopped an SSRI or SNRI. For a long window after stopping, many people still said effects felt reduced compared with the first week off meds. The paper suggests the odds of still feeling “dampened” did not shift much until roughly 3 to 6 months off (see the paper for the exact stats). Plain English: some people still feel “not back to normal” for months, not just a week or two.
They also checked whether fluoxetine (Prozac) alone drove the whole pattern because it stays in the body a long time. Removing fluoxetine from the math did not erase the pattern.
Strengths and limits
Strengths: large sample, clear stats, directly answers the “on meds / off meds” worry many people have.
Limits: memory bias, no pill counts, no lab-tested mushroom strength, and people who take mushrooms often may be over-represented. Good for big-picture odds, bad for predicting your next weekend.
Study 2: Barbut Siva et al., 2024 (survey before the trip)
Another team used prospective surveys: people filled out forms before they planned to use a classic psychedelic, then again after. Open access link: DOI 10.1177/02698811231224217.
People with a self-reported mental health diagnosis were split into currently on serotonin antidepressants (SSRI/SNRI type) versus not on those meds.
What looked different during the trip
People on meds reported less intense overall trip scores. They scored lower on:
- Mystical-type questions (about 18% lower in the stats they report)
- Emotional breakthrough questions (about 32% lower)
- People not on meds reported more “challenging” trip features in this analysis (read the paper for what “challenging” meant in their forms)
Visual scores were not clearly different between groups in the analysis they published.
What looked similar a month later
About four weeks later, both groups showed similar self-reported gains in well-being and depression scores in the models they ran. That does not prove meds are “just as good” for healing trips. It does push back on the simple story that a louder trip always means better life outcomes on a survey.
Study 3: Becker et al., 2022 (small lab study, healthy volunteers)
This one was a randomized crossover study: healthy adults got escitalopram or placebo for 14 days, then psilocybin in a controlled setting. PubMed link: 34743319.
In that setup, escitalopram cut some physical stress signals and some bad side effects from psilocybin, but the authors did not see a big drop in positive subjective effects. That can sound opposite to forum posts. Why the mismatch?
- Healthy young adults are not the same as depressed patients.
- Two weeks of one SSRI is not the same as five years on another drug.
- Hospital dosing is not the same as unknown street mushroom strength.
- Different studies measure different things (total mystical score vs “walls moved” vs heart rate).
So: meds can blunt trips in surveys, but the amount of blunting depends on the person, drug, dose, and study design.
Serotonin syndrome: what it is, and how worried to be
Serotonin syndrome means too much serotonin activity at once. It can be serious. Classic triggers are things like certain antidepressant mixes, MAOIs plus other serotonergic drugs, tramadol combos, and high doses. Symptom overview for clinicians (not for self-diagnosis): StatPearls: serotonin syndrome.
Psilocin hits serotonin receptors, so in theory risk rises if you stack many serotonergic drugs or high doses. Case reports exist; news articles can hype one story. A calmer read on one case angle: Psychiatrist.com coverage.
Simple takeaways:
- Serious interactions are possible in principle when many serotonergic drugs pile up.
- Nobody should claim serotonin syndrome “never” or “always” happens from mushrooms plus an SSRI – good counts do not exist for street use.
- If someone has high fever, bad confusion, rigid muscles, or wild blood pressure swings, treat it as an emergency and call for help.
General risk framing (not personal medical advice): what are the risks of psychedelics.
Why “just take more mushrooms” is a bad plan
If a trip feels weak, some people raise the dose. That raises risk: stronger panic, confusion, heart stress, falls, and worse outcomes for people with bipolar spectrum illness. Read psilocybin tolerance for how repeated trips stack. SSRIs are not a free pass to mega-dose.
Therapy setting vs using on your own
Legal therapy trials use screening, a therapist team, and a care plan. For how that model is supposed to work, see how psychedelic therapy works and psilocybin therapy explained. The point for meds: a medical program cares about safety first, not “max visuals.” Changing meds belongs with a psychiatrist.
Where forums and studies agree
- Blunting is common enough to take seriously.
- Time on meds and time off meds both matter.
- Not everyone gets blunted.
- In the Gukasyan numbers, SNRIs were not clearly “safer” than SSRIs for feeling a weaker trip.
Where forums and studies disagree (or we still lack data)
- “Two weeks off my SSRI is enough.” Trials use short washouts for logistics. Survey data hints some people feel “off” for months. Do not DIY a med taper from a blog.
- How often serotonin syndrome happens with psilocybin plus common SSRIs – we do not have a clean rate from street use.
- Peak trip intensity vs long-run mood help – not the same thing; surveys show you can feel less peak and still report mood gains weeks later.
If you talk to a doctor (education only)
Again: not medical advice. If you have a real visit, useful topics include: which drug and dose you take, how long you have been stable, any history of mania, psychosis, or bipolar disorder, other meds (sleep aids, ADHD stimulants, tramadol, migraine triptans, etc.), and heart or seizure history. Patient-friendly antidepressant basics: Mind UK: about antidepressants.
- If you are in crisis, call your local emergency number or a crisis line. Canada: Talk Suicide Canada.
- If you want to understand why trials pause meds, read the actual trial papers linked above, not only forum posts.
Bottom line in plain words
What people report: weaker trips on SSRIs/SNRIs, messy timelines after stopping, fear about serotonin syndrome, and random dose advice online.
What studies suggest: large surveys find weaker-than-expected trips are common on SSRIs/SNRIs, and some people still feel dampened effects for months after stopping in survey data. A newer survey found softer peak scores on meds but similar mood survey gains at four weeks in their stats. A small lab study on short-term escitalopram did not wipe out all positive effects. None of that replaces your doctor.
Forums tell one person’s story. Studies guess about averages. Your prescriber works with you.
Further reading (Shroom Bros)
- Magic mushrooms and depression
- Magic mushrooms and mental health
- Psilocybin and neuroplasticity
- Psilocybin tolerance
- Risks of psychedelics
- How psychedelic therapy works
- Microdosing 101
More guides: Magic Mushroom Blog. Always follow the laws where you live.
Buy The Best Magic Mushrooms in Canada (19+)
Sources
- Gukasyan N, Griffiths RR, Yaden DB, Antoine DG, Nayak SM, et al. Attenuation of psilocybin mushroom effects during and after SSRI/SNRI antidepressant use. J Psychopharmacol. 2023. https://doi.org/10.1177/02698811231179910
- Barbut Siva J, Barba T, Kettner H, Kuc J, Nutt DJ, Carhart-Harris RL, Erritzoe D, et al. Interactions between classic psychedelics and serotonergic antidepressants. J Psychopharmacol. 2024. https://doi.org/10.1177/02698811231224217
- Becker AM, Holze F, Grandinetti T, et al. Acute effects of psilocybin after escitalopram or placebo pretreatment. Clin Pharmacol Ther. 2022. PubMed: 34743319
- Davis AK, Barrett FS, May DG, et al. Psilocybin-assisted therapy for major depressive disorder. JAMA Psychiatry. 2021. PubMed: 33146667
- Carhart-Harris RL, Giribaldi B, Watts R, et al. Psilocybin versus escitalopram for depression. N Engl J Med. 2021. PubMed: 33852780
- NIMH. Mental health medications. nimh.nih.gov
- StatPearls. Serotonin syndrome. NCBI Bookshelf NBK482377
- Mind UK. About antidepressants. mind.org.uk
- MedlinePlus. Antidepressants. medlineplus.gov
Disclaimer: Education only. Not medical or legal advice. Laws vary. Never change psychiatric meds without your prescriber.