Most “trip sitter advice” online is either too vague (“just be supportive”) or too dramatic (“be a shaman”). In real life, the best sitters usually aren’t performing wisdom—they’re running a calm environment like a quiet stage crew while someone else is doing hard inner work.
This playbook is built for readability: 15 concrete behaviors you can actually execute, plus a few high-value add-ons—music strategy, lighting rules, when to speak, when silence wins, and what to do when the experience gets bumpy.
Disclaimer: Educational and harm-reduction information only. Not medical advice. If someone may be a danger to themselves or others, or appears medically unwell, seek emergency help.
What a Trip Sitter Is Actually Optimizing For
Altered states often amplify sensory load, social complexity, and uncertainty. Your job is to reduce those three variables without taking control of the traveler’s inner process.
Think in outcomes:
Safety: prevent injury, dehydration, wandering into unsafe situations, and medical emergencies.
Predictability: stable lighting, stable sound, stable emotional tone from you.
Agency: support their choices when they’re coherent; don’t steer their psyche.
If you remember only one line: You are not the director of the trip. You are the stage crew.
Before Anything Starts: A 10-Minute Sitter Setup (Worth It)
These aren’t “behaviors” during the trip, but they make the behaviors work:
Clean the main room (clutter reads as “noise” to a heightened brain).
Pre-stage water (easy lid, stable cup, spill-friendly placement).
Temperature check (slightly warm beats slightly cold for many people).
Bathroom clarity (door unlocked path, nightlight if needed).
Interception plan for roommates, pets, deliveries, and phones.
Also decide sober what “escalation” means for your group—when to call a trusted third person, when to seek medical help. Deciding while altered is harder.
The Playbook: 15 Concrete Behaviors
Each item below includes what to do, why it helps, and a quick common mistake to avoid.
1) Pre-brief signals and boundaries (so language doesn’t fail later)
What to do: Agree on simple signals for quiet, company, and physical contact (yes / no / ask each time). Agree whether you’ll suggest leaving the house (often best avoided unless planned).
Why it helps: At peak intensity, complex negotiation feels impossible. Signals compress decisions.
Common mistake: Vague reassurance (“I’m here if you need anything”) without concrete options.
2) Default to quiet presence during the steepest windows
What to do: During the most intense come-up/peak stretches, treat silence + availability as the default. Sit where they can see you if that comforts them—or sit nearby if they prefer eyes-closed darkness.
Why it helps: Many people become hyper-attuned to tone, subtext, and “being interpreted.” Too much talking can feel like surveillance.
Common mistake: Filling silence because you’re nervous. Your boredom is not their problem to solve.
3) Use short acknowledgments instead of speeches
What to do: Keep lines brief and repeatable: “You’re safe.”“I’m with you.”“This will pass.”
Why it helps: Long monologues add cognitive load and can sound like you’re trying to “logic” them out of an experience that isn’t primarily logical.
Common mistake: Teaching philosophy mid-peak. Even if it’s true, it’s poorly timed.
4) Ask one question at a time—never stack questions
What to do: Ask a single yes/no question: “Want a blanket?” Wait. Accept no.
Why it helps: Stacked questions force multitasking while multitasking feels broken.
Common mistake: “Do you want water or tea, are you cold, should we change the music, are you hungry?”
5) Avoid “why” questions while they’re altered
What to do: Replace “Why are you scared?” with concrete offers: lower lights, slower music, blanket, fresh air (if safe and agreed), bathroom escort.
Why it helps: “Why” prompts analysis; many people need stabilization first.
Common mistake: Investigative interviewing that accidentally turns the trip into a performance.
What to do: Prefer lamps over harsh overheads. Warm color temperature. Indirect bounce light beats pointing a bright bulb at someone’s face.
Why it helps: Visual complexity and flicker can feed loops and unease.
Common mistake: RGB color storms or strobes because they look cool online.
8) Reduce visual “noise” in the room
What to do: Hide clutter, blinking router lights, messy stacks, chaotic posters if the room feels aggressive. Close unrelated tabs on TV/laptop.
Why it helps: Pattern recognition ramps up; the environment becomes part of the content.
Common mistake: Leaving chaotic visuals up because “it’s their apartment.” You can still tidy the session space.
9) Phones silenced for everyone in the space
What to do: Silent mode, face-down, no random TikTok beside someone peaking unless they request a specific clip/song.
Why it helps: Notifications are micro-startles; startles scale badly.
Common mistake: The sitter scrolling while the traveler feels “watched.”
10) Offer water and simple food without pressure
What to do: Keep water visible and reachable. Offer simple foods (fruit, toast). If they decline, accept it calmly.
Why it helps: Dehydration and low blood sugar can worsen discomfort—but forcing intake can worsen distress.
Common mistake: Parental nagging. Offer once, wait, offer later.
11) Bathroom support: respectful proximity
What to do: If they want help, many people prefer you wait outside the door (unless you’ve agreed otherwise). Keep instructions simple: “I’m right here.”
Why it helps: Bathrooms can feel disorienting; proximity reduces panic without crowding.
Common mistake: Jokes or playful commentary while they’re vulnerable.
12) Treat temperature as a first-line intervention
What to do: Socks, blanket, room temp tweak, offer a warm mug to hold (even herbal tea if appropriate).
Why it helps: Cold hands/feet can cascade into somatic worry.
Common mistake: Ignoring physical discomfort while trying to talk them through it.
13) If distress rises, change one channel at a time
What to do: Choose one lever: music OR lighting OR room change OR fresh air (if safe). Wait a few minutes. Reassess.
Why it helps: Multiple simultaneous changes can feel like the world is “escalating.”
Common mistake: Panic-redesigning the entire environment in five minutes.
14) Validate emotions without arguing about content
What to do: Reflect the feeling: “That sounds overwhelming.” Stabilize the body: “You’re safe here.” Offer a concrete next step: “Want the lights lower?”
Why it helps: Debating unusual thoughts mid-trip rarely resolves them—and can increase shame.
Common mistake: Fact-checking their perceptions like a courtroom.
15) Know the emergency threshold—and use it if needed
What to do: If you see signs of medical emergency, self-harm, violence, or a sustained inability to stay oriented that isn’t improving with calm support, call emergency services. A sitter’s job includes real-world safety, not “handling everything in-house.”
Why it helps: Some situations are not psychological “difficulty”—they’re emergencies.
Common mistake: Pride. Don’t risk someone’s life to avoid “making a scene.”
Quick Reference: When to Speak vs When to Stay Quiet
Situation
Default move
What to say (examples)
Peak intensity, eyes closed
Quiet presence
(none unless spoken to)
They ask a direct question
Short honest answers
“Yes.” / “I don’t know.” / “In about an hour, usually.”
Fear without a clear request
Stabilize body + environment
“You’re safe. I’m here. Want a blanket?”
Looping questions
Same calm answer each time
Don’t improvise new explanations every loop
They want connection
Gentle conversation at their pace
Follow their topic; don’t redirect to your agenda
Handling Common Bumpy Moments (Short Playbooks)
Nausea or GI discomfort
Reduce smells (food prep, incense).
Offer water; keep a bin nearby just in case.
Calm, boring posture from you—no frantic energy.
Time distortion (“Is it forever?”)
Don’t debate time philosophically.
Offer a simple anchor: “It’s been about X minutes since you took it.” (Only if you actually know.)
Paranoia directed at you (“You’re plotting”)
Lower defensiveness. Slow voice.
Offer transparency + choice: “I can sit farther away. Want me outside the door?”
They want the music off—then silence feels too loud
Try ultra-soft ambient bed at very low volume, or gentle room tone (fan/hum) if available—still no surprises.
Three “Pro Moves” That Separate Good Sitters from Great Ones
A) You regulate your own nervous system on purpose
Slow breathing, slower movements, softer volume, wider gaps between sentences. Your physiology is contagious.
B) You manage logistics like a professional
Doorbells, pets, roommates, food delivery—intercept the outside world so the traveler doesn’t have to negotiate reality.
C) You save debriefing for later
Mid-trip “meaning extraction” can pressure people. Notes are fine; deep analysis is often better after sleep.
Optional: A Small “Sitter Bag” (Simple Items)
Electrolyte packets + water
Light snacks (plain, low odor)
Wet wipes / tissues
Clean socks
Eye mask (only if they want it)
Charging cable (for their phone if needed—used minimally)
Frequently Asked Questions
Should the sitter be completely sober?
For best judgment and safety, yes. The sitter is the baseline anchor.
What if they want me to talk the whole time?
Follow their lead—but keep your turns shorter than usual. Let them steer topics.
What if I’m getting overwhelmed?
Tag in a second sober person if possible. If not, slow your body down first (breath, shoulders), then simplify the environment.
The Bottom Line
Great trip sitting is mostly boring competence: predictable environment, gentle voice, short sentences, thoughtful music, stable lighting, and the wisdom to stay quiet while someone navigates the experience.
If you’ve ever stared at a chocolate bar wrapper and thought, “So… how much is one square?”—you’re not overthinking it. You’re doing the right kind of thinking.
Psilocybin edibles are convenient, but the math behind them is surprisingly easy to get wrong—because the label is rarely the whole story. This guide explains the framework for edible dosing math: what brands often mean by grams, how that relates to psilocybin content in theory, why homogeneity matters, and why your body doesn’t behave like a calculator.
Important: This is general education, not dosing advice. Psilocybin is regulated in many places; only follow applicable laws. Never drive impaired. If you have health questions, ask a qualified clinician.
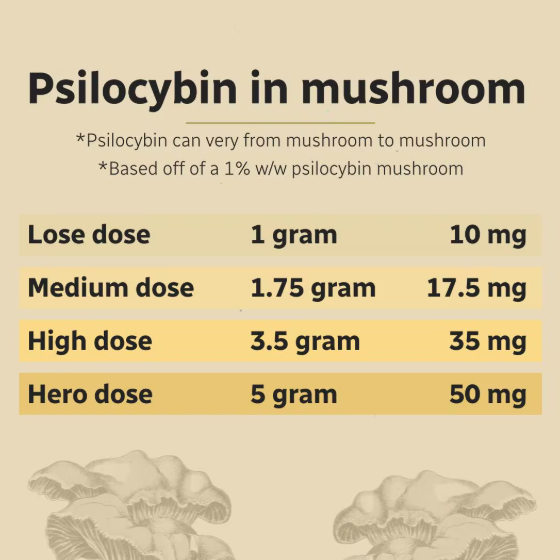
1. The First Rule: “Grams on the Label” Usually Means Mushroom Material, Not Pure Psilocybin
Many mushroom edibles advertise a total like “3.5 g” or “1 g per piece.” In most cases, that number is best read as grams of mushroom material (or extract equivalent) used in the recipe—not grams of the chemical psilocybin.
Why that distinction matters:
Pure psilocybin is measured in milligrams (mg).
Dried mushrooms are mostly fiber, water (when fresh), chitin, and other compounds—only a small fraction is psilocybin.
So if your brain automatically converts “3.5 g” into “3.5 g of drug,” you’ll be off by orders of magnitude.
2. The “Mushroom Gram → Psilocybin mg” Step Is the Leaky Part of the Math
People sometimes try to estimate psilocybin milligrams from dried weight using a rough potency assumption. In the real world, potency swings with species/variety, growing conditions, storage, dehydration method (freeze-dried vs air-dried), and age.
That means any “mg per gram of dried mushroom” figure should be treated as a wide uncertainty band, not a constant.
Practical takeaway: edible math is less like precision engineering and more like budgeting with a volatile exchange rate. The label gives you a reference point; it does not guarantee what your liver will see.
3. How to Read a Bar: Total Content ÷ Number of Pieces
If a product states a total mushroom weight for the entire package, the simplest structure is:
Per piece (labeled mushroom basis) ≈ Total stated grams ÷ Number of pieces
Example structure (illustrative only): If a bar is marketed as containing 3.5 g total mushroom material and has 10 squares, then each square represents about 0.35 g of that labeled mushroom basis—if the infusion is even.
That “if” is doing a lot of work. Which brings us to homogeneity.
4. Homogeneity: The Hidden Variable That Breaks Neat Math
Even perfect division on paper fails if the active ingredient isn’t evenly distributed. In kitchens and small-batch production, uneven mixing is a common failure mode.
What unevenness feels like in practice: two pieces from the same bar, same “math,” different intensity.
Harm-reduction implication: treat early samples cautiously, especially with a new batch or a new supplier—even if you “did the math.”
5. Gummies vs Chocolate: Same Label, Different Delivery Story
Chocolate (often contains fat)
Fats can influence how quickly your body processes what you ate—alongside stomach contents and individual metabolism.
People often report differences in onset and “curve shape” compared with eating dried mushrooms.
6. “Extract Equivalents” vs Whole Mushroom: Labels Can Mean Different Things
Some products are built from concentrates or extracts. A label might still speak in “dried gram equivalent” language—or it might not translate cleanly to what you’re picturing.
What to look for on packaging (when available):
Whether the number refers to input material, equivalent, or something else
Whether the product claims homogeneity or batch testing (not all markets require this)
Whether pieces are scored consistently
If the label is ambiguous, the only safe assumption is: variance is higher than you want it to be.
7. Onset Math Isn’t the Same as Peak Math
Even if you had perfect milligram knowledge (you usually don’t), onset depends on:
What else you ate
GI transit time
Sleep, hydration, stress
Individual enzyme and metabolism differences
So the common mistake is: re-dosing too early because “the math says it should have worked by now.” With edibles, patience isn’t just a virtue—it’s a safety tool.
8. A Sensible “Spreadsheet Mindset” Without Pretending Precision
If you like structured thinking, use three columns—not to claim precision, but to track uncertainty:
Label basis: total stated mushroom basis per package
Geometry basis: pieces per package → per-piece basis
Most bad outcomes come from trusting column 2 while ignoring column 3.
9. Why “Tolerance” and “Set/Setting” Change the Experience Even If the Math Stays Constant
Two days with the same calculated intake can feel different because your nervous system isn’t a fixed instrument. Tolerance, sleep debt, anxiety, environment, and co-used substances (including alcohol and cannabis) can change subjective intensity and side effects.
10. Storage Math: Potency Changes Over Time (Slowly, but Real)
Heat, oxygen, and moisture are not friends to stable storage. Poor storage doesn’t just “ruin the vibe”—it can change how reliable your expectations are from piece to piece over weeks.
Can I convert chocolate bar “grams” into milligrams of psilocybin accurately?
Usually, no—not from packaging alone. Without verified testing for that batch, you’re estimating inside a wide band.
Why did half a bar hit harder than a full bar last month?
Different batch, different storage, different stomach contents, different tolerance—or uneven distribution within the product.
Is “start low, go slow” still the answer if I’m good at math?
Yes—because the limiting factor is rarely arithmetic; it’s biological and manufacturing variability.
Does lemon tekking logic apply to edibles?
Not cleanly. Edibles are a different route and matrix. For lemon tek concepts with mushrooms, see: Lemon Tek: The Ultimate Guide.
The Bottom Line
Edible dosing “math” is really two problems stacked together: (1) what the label means, and (2) how evenly and predictably that meaning shows up in real life. Get the definitions right, divide carefully, assume variance, and treat onset as a window—not a countdown.
For more, browse our Magic Mushroom Blog and our edible categories in the shop—always in compliance with the law in your jurisdiction.
Last updated: April 2026 · For adults 19+ in Canada · Informational only · Not medical or legal advice
DMT Vape vs Raw DMT in a Bong: What Is Different, What Is Riskier, and What People Should Know
Medical and legal disclaimer: This article is for education and harm reduction only. It is not medical advice, legal advice, or a recommendation to use any illegal substance. DMT is controlled in many places, including Canada outside specific exemptions. Do not drive, work, or make high-risk decisions while impaired.
Quick summary: A DMT vape and raw DMT in a bong can both produce very intense effects, but they differ in consistency, heat control, respiratory stress, and how quickly intensity can escalate. A vape is often described as more repeatable and easier to titrate. A bong setup is often described as harsher, less predictable, and easier to over- or under-heat. Neither method is risk-free.
If you are researching DMT methods, the most useful question is not “which is stronger?” It is “which setup introduces fewer unknowns and fewer avoidable harms?” This guide compares the two in plain language and explains where people get into trouble.
DMT vape (pre-mixed liquid in a cartridge with a battery)
Raw/freebase DMT in a bong-style setup (solid material vaporized using a manual heat source)
Both routes are inhaled and both can become overwhelming very fast. The differences are mostly about control, consistency, and side effects from poor heat handling.
Big difference #1: Heat control and chemical stability
DMT needs to be vaporized in a useful temperature window. Too cool and effects can feel weak. Too hot and material can burn or degrade, creating a harsh inhale and wasted product.
With many vapes, heat is more stable because the battery and coil are built for repeatable output. With bong-style manual heating, heat can swing a lot from one attempt to the next, depending on flame distance, timing, airflow, and user technique.
Plain English: a vape often gives more repeatable vapor conditions; manual bong heating often has more room for error.
Big difference #2: Dose consistency and escalation speed
People often report that vapes allow smaller, more gradual inhalations with less setup friction. That can feel easier to pace. But because the process is easy, people may take repeated pulls quickly and accidentally escalate intensity.
With raw DMT in a bong-style setup, each attempt can vary more. That variability can produce either weak attempts or sudden heavy effects when conditions line up. Inconsistent delivery is one reason people describe this route as less predictable.
Takeaway: “easier to use” does not mean “low risk.” It often means intensity can build before a person notices how far they have gone.
Big difference #3: Lung and throat irritation
Respiratory irritation is a common complaint. Harsher vapor is more likely when material overheats or burns. In real-world reports, manual high-heat setups are more often linked with burning sensation, coughing, chest discomfort, and unpleasant taste.
Cartridge vapor is not harmless, but many users describe it as smoother and less physically punishing than poorly heated raw setups. Device quality, liquid formulation, and contamination still matter.
Important: if someone already has asthma, bronchitis, COPD, or other lung issues, inhaled psychoactives can raise risk.
Big difference #4: Practical safety around impairment
DMT effects can begin very fast. A person may lose motor control, awareness of surroundings, or ability to communicate within seconds to minutes. That creates immediate physical safety risks (falls, burns, dropping hot objects, panic movement).
Manual bong-style heating introduces extra hazards before and during onset: open flame, hot glass, and more complex handling. A vape may remove open flame risk, but it does not remove impairment risk.
Manual heat route: more burn and handling hazards.
Vape route: fewer flame hazards, but still very high impairment risk.
Big difference #5: Reliability of what is actually in the product
Raw crystal and cartridges both carry quality uncertainty in unregulated markets. With cartridges, people cannot easily verify concentration, cutting agents, or contamination without proper lab testing. With raw material, purity and identity can still be uncertain.
This is one of the biggest blind spots in all online method debates. People compare “device A vs device B” while ignoring that unknown chemistry can dominate the outcome.
What users usually mean by “vape is easier”
When people say vapes are easier, they usually mean:
Less setup complexity
Less heat guesswork
Fewer failed attempts from overheating
Less harsh throat hit (for many users)
That does not mean the psychological experience is easy. DMT can still be disorienting, intense, and emotionally destabilizing regardless of device type.
What users usually mean by “raw in a bong hits harder”
Some people say bong-style delivery feels “harder” or more abrupt. In many cases, that impression is a mix of:
Sudden delivery when technique happens to line up
Harshness and cough being interpreted as intensity
Large variation between attempts (one weak, next very strong)
So “harder” does not always mean “better delivery.” Sometimes it means more chaotic delivery.
Mental health risks do not disappear with any device
No device removes core psychedelic mental risks. People with personal or family history of psychosis, bipolar mania, severe panic disorder, or unstable mood may face higher risk from very intense experiences.
Even in people without diagnosed conditions, short intense states can trigger panic, derealization, confusion, and distress afterward. Device choice changes logistics – not fundamental neuropsychological risk.
Mixing psychoactives raises unpredictability. Combining with alcohol, cannabis, stimulants, or multiple serotonergic drugs can amplify confusion and physical stress. If someone is on psychiatric medication, interaction risk should be discussed with a clinician, not guessed from forums.
For antidepressant interaction context, see your internal guide on SSRIs/SNRIs and psilocybin. The broader point still applies here: mixed-substance states are harder to predict and manage.
Harm-reduction baseline (non-technical)
This is not a how-to section. It is a risk-minimization baseline:
Do not use alone.
Do not combine with driving, tools, heights, water, or fire.
Avoid stacking substances.
If someone has chest pain, severe confusion, breathing trouble, or dangerous behavior, seek emergency help.
Safer planning is always less dramatic and less impulsive than internet highlight clips.
Simple comparison table (plain language)
Consistency: Vape usually more repeatable; manual bong route more variable.
Heat control: Vape usually easier; manual route easier to overheat.
Harshness: Manual route often harsher if heat is off.
Mental intensity risk: High for both; neither is psychologically “safe.”
Unknown product risk: Present in both when unregulated.
FAQ
Is a DMT vape safer than raw DMT in a bong?
It may reduce some mechanical risks (open flame, rough heat swings), but it does not remove core impairment or mental health risks. “Safer” is relative, not absolute.
Why do people say the bong method is harsher?
Mostly heat control issues. Overheating can produce a rough inhale and cough, which many people describe as harsh or unpleasant.
Which one is stronger?
Strength depends on many factors: concentration, heat, inhalation pattern, individual sensitivity, and product quality. Device type alone does not determine outcome.
Can I trust forum dosing claims?
Not as medical or safety guidance. Forum reports are anecdotal and often leave out key details.
DMT vape vs raw DMT in a bong is mostly a question of consistency and avoidable hazards, not a question of one route being harmless. Vapes are often seen as easier and more repeatable. Manual bong setups are often seen as harsher and more variable. Both can become overwhelming quickly, and both carry legal, physical, and mental health risks.
If your goal is informed decision-making, prioritize verified information, conservative planning, and safety over intensity chasing.
Last updated: April 2026 · For adults 19+ in Canada · Informational only · Not medical advice
Psilocybin and SSRIs/SNRIs: What People Report vs What Studies Suggest
Medical disclaimer: This article is for general education only. It is not medical advice. It is not telling you to start, stop, or change any medication or drug. Changing antidepressants can be risky (withdrawal, relapse). Talk to your prescribing doctor about your own situation.
Quick summary: Many people on SSRIs or SNRIs say psilocybin feels weaker. Big surveys and some lab studies back that up. No one can promise what will happen to you. Do not raise your dose to “make up” for blunting – that can be dangerous.
If you want to know how psilocybin (the active ingredient in magic mushrooms) might interact with SSRIs and SNRIs, you are not alone. Forums are full of personal stories. Researchers run surveys and clinical trials. Both are useful, but they answer different questions.
SSRIs stand for selective serotonin reuptake inhibitors. Common examples include sertraline (Zoloft), escitalopram (Lexapro), and fluoxetine (Prozac). They mostly work by helping the brain keep more serotonin available. Doctors often prescribe them for depression and anxiety.
SNRIs are serotonin-norepinephrine reuptake inhibitors. Examples include venlafaxine (Effexor) and duloxetine (Cymbalta). They affect serotonin and another chemical called norepinephrine.
What is psilocybin doing in the brain? (Still simple)
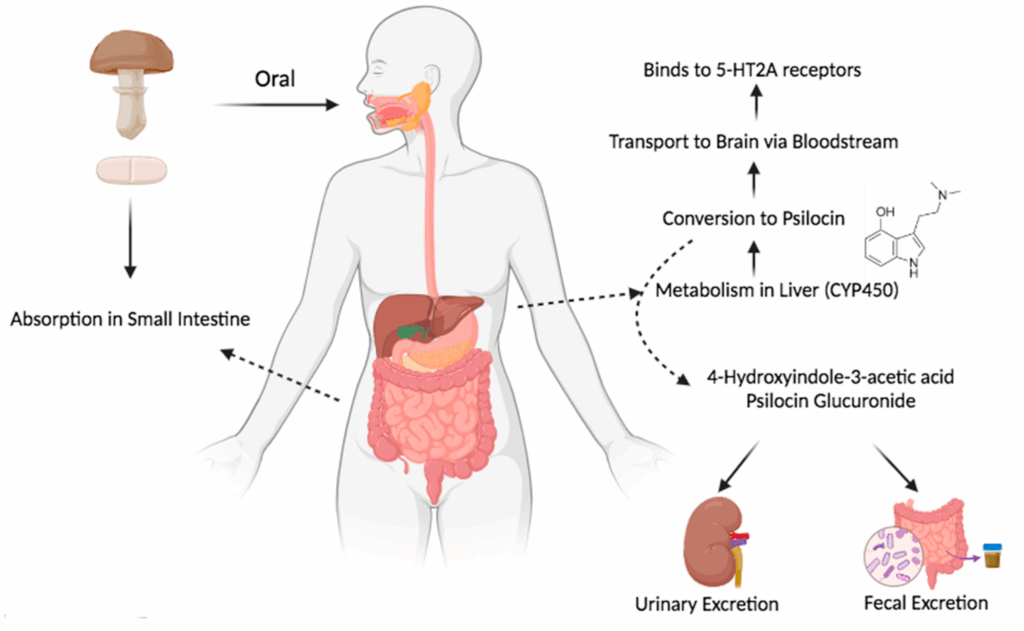
Psilocybin turns into psilocin in the body. Psilocin attaches to certain serotonin receptors, especially 5-HT2A. That receptor is part of why people see shifts in perception, mood, and thinking during a trip. For a longer read on brain change after mushrooms, see psilocybin and neuroplasticity.
Because antidepressants also touch the serotonin system (in a different way than psilocin), scientists always wondered if mixing the two could dull or change a trip.
Why research studies often ask people to stop antidepressants first
In many psilocybin therapy trials, people are asked to taper off serotonergic antidepressants and wait a washout period before a study dose. Reasons include safety, clearer results, and older data suggesting meds can blunt psychedelic effects.
Important: What a study protocol allows is not the same as what is safe for random home use. Trials have doctors, fixed doses, and rules. Real life has mixed drugs, unknown mushroom strength, alcohol or cannabis on the side, and no nurse in the room.
What people say online (patterns, not proof)
Reddit threads are not a random sample. People with wild stories post more than people with boring nights. Still, the same lines show up a lot. Think of these as themes, not facts.
“My trip felt weaker on my SSRI.” Often same product and dose as before, but less intensity or shorter peak.
“I stopped my SSRI for a week and it still felt weak.” People argue about how long blunting lasts.
“I tripped hard on an SNRI anyway.” Bodies differ. Dose, genetics, liver health, batch strength, and setting all matter.
“Will I get serotonin syndrome?” Some threads panic. Others say “never happens.” The truth is calmer and more careful than both (see below).
Microdosing while medicated. Stories are mixed. For basics on microdosing (not drug interaction advice), read microdosing 101 and what is microdosing.
Compared with studies, online posts usually lack hard details: no blood levels, no lab-tested mushroom dose, no list of other drugs taken that night.
Study 1: Gukasyan et al., 2023 (big survey after the fact)
Researchers ran a large online survey of people who had used psilocybin mushrooms while on an antidepressant and/or within two years after stopping one. Full paper: DOI 10.1177/02698811231179910 (Journal of Psychopharmacology).
While still on medication
There were 611 reports of using mushrooms while on an antidepressant. People compared how strong the trip felt versus what they expected. Rough odds of weaker than expected effects:
About 47% (SSRIs) – think “nearly half”
About 55% (SNRIs) – a bit higher than SSRIs in this survey
About 29% (bupropion) – bupropion is a different kind of antidepressant, not a classic SSRI/SNRI
So: weaker trips on meds are common in this data set. That does not mean everyone feels nothing.
After stopping medication
There were 1,542 reports after people stopped an SSRI or SNRI. For a long window after stopping, many people still said effects felt reduced compared with the first week off meds. The paper suggests the odds of still feeling “dampened” did not shift much until roughly 3 to 6 months off (see the paper for the exact stats). Plain English: some people still feel “not back to normal” for months, not just a week or two.
They also checked whether fluoxetine (Prozac) alone drove the whole pattern because it stays in the body a long time. Removing fluoxetine from the math did not erase the pattern.
Strengths and limits
Strengths: large sample, clear stats, directly answers the “on meds / off meds” worry many people have.
Limits: memory bias, no pill counts, no lab-tested mushroom strength, and people who take mushrooms often may be over-represented. Good for big-picture odds, bad for predicting your next weekend.
Study 2: Barbut Siva et al., 2024 (survey before the trip)
Another team used prospective surveys: people filled out forms before they planned to use a classic psychedelic, then again after. Open access link: DOI 10.1177/02698811231224217.
People with a self-reported mental health diagnosis were split into currently on serotonin antidepressants (SSRI/SNRI type) versus not on those meds.
What looked different during the trip
People on meds reported less intense overall trip scores. They scored lower on:
Mystical-type questions (about 18% lower in the stats they report)
People not on meds reported more “challenging” trip features in this analysis (read the paper for what “challenging” meant in their forms)
Visual scores were not clearly different between groups in the analysis they published.
What looked similar a month later
About four weeks later, both groups showed similar self-reported gains in well-being and depression scores in the models they ran. That does not prove meds are “just as good” for healing trips. It does push back on the simple story that a louder trip always means better life outcomes on a survey.
Study 3: Becker et al., 2022 (small lab study, healthy volunteers)
This one was a randomized crossover study: healthy adults got escitalopram or placebo for 14 days, then psilocybin in a controlled setting. PubMed link: 34743319.
In that setup, escitalopram cut some physical stress signals and some bad side effects from psilocybin, but the authors did not see a big drop in positive subjective effects. That can sound opposite to forum posts. Why the mismatch?
Healthy young adults are not the same as depressed patients.
Two weeks of one SSRI is not the same as five years on another drug.
Hospital dosing is not the same as unknown street mushroom strength.
Different studies measure different things (total mystical score vs “walls moved” vs heart rate).
So: meds can blunt trips in surveys, but the amount of blunting depends on the person, drug, dose, and study design.
Serotonin syndrome: what it is, and how worried to be
Serotonin syndrome means too much serotonin activity at once. It can be serious. Classic triggers are things like certain antidepressant mixes, MAOIs plus other serotonergic drugs, tramadol combos, and high doses. Symptom overview for clinicians (not for self-diagnosis): StatPearls: serotonin syndrome.
Psilocin hits serotonin receptors, so in theory risk rises if you stack many serotonergic drugs or high doses. Case reports exist; news articles can hype one story. A calmer read on one case angle: Psychiatrist.com coverage.
Simple takeaways:
Serious interactions are possible in principle when many serotonergic drugs pile up.
Nobody should claim serotonin syndrome “never” or “always” happens from mushrooms plus an SSRI – good counts do not exist for street use.
If someone has high fever, bad confusion, rigid muscles, or wild blood pressure swings, treat it as an emergency and call for help.
If a trip feels weak, some people raise the dose. That raises risk: stronger panic, confusion, heart stress, falls, and worse outcomes for people with bipolar spectrum illness. Read psilocybin tolerance for how repeated trips stack. SSRIs are not a free pass to mega-dose.
Therapy setting vs using on your own
Legal therapy trials use screening, a therapist team, and a care plan. For how that model is supposed to work, see how psychedelic therapy works and psilocybin therapy explained. The point for meds: a medical program cares about safety first, not “max visuals.” Changing meds belongs with a psychiatrist.
Where forums and studies agree
Blunting is common enough to take seriously.
Time on meds and time off meds both matter.
Not everyone gets blunted.
In the Gukasyan numbers, SNRIs were not clearly “safer” than SSRIs for feeling a weaker trip.
Where forums and studies disagree (or we still lack data)
“Two weeks off my SSRI is enough.” Trials use short washouts for logistics. Survey data hints some people feel “off” for months. Do not DIY a med taper from a blog.
How often serotonin syndrome happens with psilocybin plus common SSRIs – we do not have a clean rate from street use.
Peak trip intensity vs long-run mood help – not the same thing; surveys show you can feel less peak and still report mood gains weeks later.
If you talk to a doctor (education only)
Again: not medical advice. If you have a real visit, useful topics include: which drug and dose you take, how long you have been stable, any history of mania, psychosis, or bipolar disorder, other meds (sleep aids, ADHD stimulants, tramadol, migraine triptans, etc.), and heart or seizure history. Patient-friendly antidepressant basics: Mind UK: about antidepressants.
If you are in crisis, call your local emergency number or a crisis line. Canada: Talk Suicide Canada.
If you want to understand why trials pause meds, read the actual trial papers linked above, not only forum posts.
Bottom line in plain words
What people report: weaker trips on SSRIs/SNRIs, messy timelines after stopping, fear about serotonin syndrome, and random dose advice online.
What studies suggest: large surveys find weaker-than-expected trips are common on SSRIs/SNRIs, and some people still feel dampened effects for months after stopping in survey data. A newer survey found softer peak scores on meds but similar mood survey gains at four weeks in their stats. A small lab study on short-term escitalopram did not wipe out all positive effects. None of that replaces your doctor.
Forums tell one person’s story. Studies guess about averages. Your prescriber works with you.
Gukasyan N, Griffiths RR, Yaden DB, Antoine DG, Nayak SM, et al. Attenuation of psilocybin mushroom effects during and after SSRI/SNRI antidepressant use. J Psychopharmacol. 2023. https://doi.org/10.1177/02698811231179910
Barbut Siva J, Barba T, Kettner H, Kuc J, Nutt DJ, Carhart-Harris RL, Erritzoe D, et al. Interactions between classic psychedelics and serotonergic antidepressants. J Psychopharmacol. 2024. https://doi.org/10.1177/02698811231224217
Becker AM, Holze F, Grandinetti T, et al. Acute effects of psilocybin after escitalopram or placebo pretreatment. Clin Pharmacol Ther. 2022. PubMed: 34743319
Davis AK, Barrett FS, May DG, et al. Psilocybin-assisted therapy for major depressive disorder. JAMA Psychiatry. 2021. PubMed: 33146667
Carhart-Harris RL, Giribaldi B, Watts R, et al. Psilocybin versus escitalopram for depression. N Engl J Med. 2021. PubMed: 33852780
After a psilocybin session, one of the most practical questions people ask is deceptively simple: When is it okay to drive?
The honest answer is not a catchy number of hours. It is a chain of facts: psilocybin impairs the same capacities that safe driving depends on—visual processing, attention, reaction time, and judgment—long after the “peak” feels finished. Sleep, residual effects, and how you feel the next morning all matter.
This article is for education and harm reduction. It is not telling you to drive after any substance. In Canada, driving impaired by drugs (including psilocybin) is illegal and dangerous. If you are not completely sober and unimpaired, do not drive—use a taxi, rideshare, transit, or a sober driver.
Let’s break down what the science and real-world patterns suggest about timing, sleep, afterglow, and next-day focus—so you can plan responsibly.
First: Why “How Many Hours?” Is the Wrong Starting Point
Driving requires sustained attention, stable perception (especially at night), quick motor responses, and sound judgment. Classical psychedelics like psilocybin disrupt those functions through agonism at the serotonin 5-HT2A receptor—the same receptor class implicated in the perceptual and cognitive changes studied in modern neuroimaging research on psilocybin.
That matters for driving because impairment is not only “seeing trails.” It can be:
Altered depth perception and contrast sensitivity
Slower or fragmented attention under cognitive load
Emotional lability or anxiety spikes in unfamiliar situations (traffic, weather, pedestrians)
Fatigue after hours of sympathetic arousal and mental intensity
So the goal is not to find the minimum hours until you “feel sort of normal.” The goal is to avoid operating heavy machinery until you are fully back to baseline—and for many people, that means not the same calendar day, and often not until after a full night’s sleep.
What Psilocybin Does in the Body (Briefly)
Psilocybin is a prodrug: it is converted to psilocin, which is responsible for most psychoactive effects. Psilocin acts as a serotonin 5-HT2A agonist (among other actions), producing dose-dependent changes in perception, cognition, and mood—effects that overlap strongly with capacities that regulators and road-safety science associate with impaired driving risk.
Acute subjective effects for many users fall into a rough window of about 4–6 hours for a full-dose experience, with meaningful individual variation based on dose, route of administration, stomach contents, individual metabolism, and set/setting. For a general timeline of onset, peak, and comedown, see our guide: How Long Do Shrooms Last?
But “the trip ended” does not automatically mean “safe to drive.” Subtle effects—emotional afterglow, mild visual “sparkle,” slowed cognition, or fatigue—can persist longer than the obvious psychedelic phase.
The Same-Day Driving Question: A Harm-Reduction Default
If you are looking for a practical default that prioritizes safety and legal risk reduction:
Do not drive during the acute effects or the comedown.
Do not drive the same day as a full-dose psilocybin session if there is any doubt about your baseline.
Plan ahead: arrange transportation before the experience begins.
Why so conservative? Because public roads mix unpredictability (other drivers, pedestrians, weather) with high stakes. Psilocybin’s effects are not reliably linear—people can feel “clear enough” while still having measurable cognitive and perceptual changes. If your goal is responsible use, separate the session from driving entirely.
Sleep After Psilocybin: Why It’s Often the Real Bottleneck
Even when subjective effects fade, people often report:
Difficulty falling asleep for many hours after ingestion
Restless or shallow sleep if sleep happens too early
That matters for driving because sleep deprivation itself impairs reaction time and attention in ways that can resemble intoxication. A person who finishes a late-night session with little sleep may be impaired the next morning even if psilocybin is no longer pharmacologically “active” in the way it was at hour three.
Practical takeaway: treat “I slept poorly” as a reason to delay driving until you are genuinely rested—not merely “awake.”
Residual Effects & Afterglow: When You Feel “Fine” But Aren’t Baseline
Many users describe an afterglow: improved mood, openness, emotional sensitivity, or a sense of clarity the day after. That can feel pleasant—and it can still coincide with:
Reduced tolerance for stress or overstimulation
Emotional sensitivity that can spike in conflict or surprise situations
Subtle perceptual changes in some individuals (especially in low light)
Afterglow is not the same as “zero impairment.” It is a different state than ordinary baseline, even when it feels positive.
Also worth naming carefully: a small minority of people report longer-lasting visual phenomena or perceptual oddities after psychedelic use. If anything like that is present, driving is inappropriate until resolved—and if symptoms persist, that’s a reason to seek qualified medical advice.
Next-Day Focus: What People Notice (and Why It Varies)
Some people report sharp focus the day after; others feel foggy, tired, or emotionally raw. Contributing factors often include:
Sleep quantity and quality
Hydration and food during/after the session
Stress level of the experience itself (beautiful but intense sessions can still deplete you)
Co-use of other substances (including alcohol or cannabis), which can compound impairment and sleep disruption
If your next-day goal includes work, childcare, or travel, plan conservatively. And if your next-day includes driving, the conservative standard is: you should feel completely normal in attention, reaction, and emotional regulation—not “good enough.”
Legal Reality in Canada (High Level)
In Canada, law enforcement can investigate drug-impaired driving using standardized field sobriety testing and drug screening technologies where applicable. The practical point for readers is simple: impaired driving is a serious criminal offence, and “I waited X hours” is not a reliable defence if you are impaired.
This article cannot interpret your personal legal risk; it can only emphasize that sobriety for driving means unimpaired, not “mostly down.”
If You Must Travel: Safer Alternatives to Driving
Sober driver arranged in advance
Rideshare/taxi
Transit where available
Stay overnight where you are, if possible
The best trip is the one that never puts you in a position to make a high-stakes decision while altered—or while sleep-deprived after being altered.
Quick Comparison: Why Psilocybin Is Not “Like Having a Beer” for Driving
People sometimes compare drugs using social drinking as a mental model. That model fails here for several reasons: psychedelic impairment can be perceptual and cognitive in ways that don’t feel like “intoxication” in the alcohol sense; confidence is unreliable; and the duration curve doesn’t match a simple blood-alcohol style decline for many users.
So don’t translate the experience into a false sense of readiness. If you’re asking whether you’re okay to drive, that uncertainty itself is a signal to wait.
Frequently Asked Questions
Is there a standard number of hours after psilocybin when driving is safe?
There is no universally safe number. Effects vary by dose, individual, route, sleep, and co-use. Harm-reduction planning should assume no same-day driving for full-dose experiences unless you have a rigorous, personal baseline—and even then, many people choose next-day-only as a rule.
Can I drive the morning after if I slept?
Sleep helps, but it is not automatic proof of fitness to drive. If you slept poorly, feel foggy, or feel emotionally unsettled, delay. If you feel completely baseline, you still must ensure you are not impaired.
Does microdosing change the driving answer?
If a person is taking any amount of a psychoactive substance that could impair attention or perception, driving may be unsafe and illegal. Many people treat microdosing as incompatible with driving for the same reasons—especially because “sub-perceptual” is subjective.
What if I feel totally sober?
Feeling sober is not always reliable. If there is any residual visual strangeness, slowed thinking, or strong emotional volatility, do not drive.
Psilocybin can be profound. It can also leave you tired, emotionally open, perceptually altered, or sleep-deprived—any of which can make driving unsafe even when the main effects seem over.
The clearest harm-reduction message is also the least glamorous: keep driving out of the equation until you are fully rested, fully baseline, and certain you are unimpaired—and when planning a session, assume you will not be the one behind the wheel that day.
Explore more educational guides on our Magic Mushroom Blog, and browse our shop responsibly in line with the laws that apply to you.
Nichols, D.E. — Psilocybin and serotonin 5-HT2A receptor pharmacology (classic psychedelic mechanism overview). Peer-reviewed reviews and chapters on psychedelic pharmacology.
Carhart-Harris, R.L. et al. — Psilocybin neuroimaging and network neuroscience (context for perceptual/cognitive effects). See e.g. Proceedings of the National Academy of Sciences and related work from Imperial College London’s Centre for Psychedelic Research.
Health Canada — Psilocybin and public health framing (legal status and health information): search Health Canada for current psilocybin-related pages.
Disclaimer: This article is for general education and harm reduction. It is not medical or legal advice. Psilocybin is regulated/illegal in many contexts; laws vary by jurisdiction. Never drive impaired. If you have health concerns, consult a qualified professional.
Most people know LSD as the drug that makes you see things. Fractals. Trails. Colours bleeding into one another. The walls breathing.
But that description — while not wrong — barely scratches the surface of what’s actually happening inside your skull when lysergic acid diethylamide enters your bloodstream and begins its long, strange, systematically documented takeover of your brain’s most fundamental functions.
This post is not about whether you should take LSD. It’s about what happens when you do — at a neurological level, hour by hour, from the moment a tab dissolves under your tongue to the lingering glow that remains the following morning.
Because what LSD does to the human brain is, from a purely scientific perspective, one of the most extraordinary pharmacological events we have ever documented. And the science behind it — from Imperial College London’s landmark neuroimaging studies to the latest 2025 research on brain network restructuring — tells a story that is far more nuanced, and far more fascinating, than anything the pop-culture version of acid ever suggested.
Let’s break it down.
First: Why Does LSD Do Anything At All?
Before the timeline, a critical foundation: why is LSD so powerful, and why does it last so absurdly long?
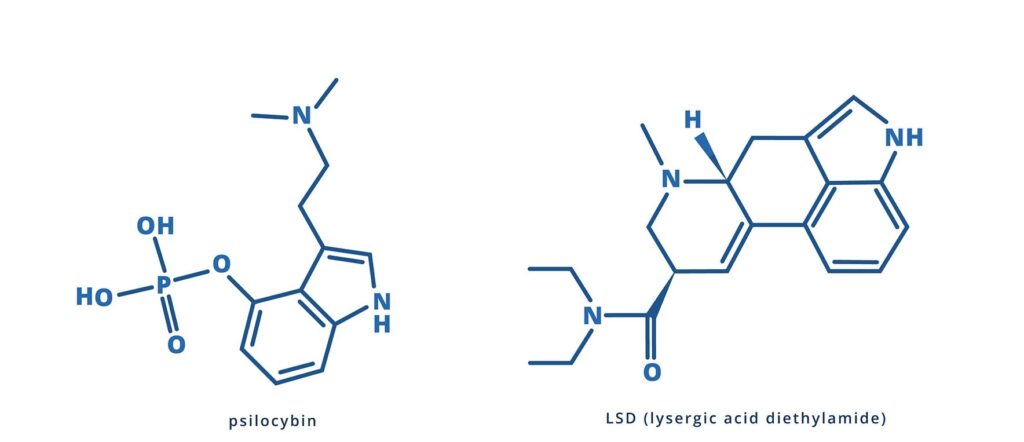
LSD — lysergic acid diethylamide — was first synthesized in 1938 by Swiss chemist Albert Hofmann, who discovered its psychedelic effects accidentally five years later after absorbing a small amount through his fingertips. It remains one of the most potent psychoactive substances ever discovered. A typical recreational dose is measured in micrograms — millionths of a gram — yet produces an experience that can last 8 to 12 hours and alter the trajectory of a person’s life.
The mechanism begins with receptor binding. LSD is a non-selective serotonin receptor agonist — it binds to most serotonin receptor subtypes in the brain, with its primary psychedelic effects mediated through the 5-HT2A receptor. These receptors are concentrated in the prefrontal cortex, the thalamus, and several other higher-order cortical regions. When LSD activates them, it triggers a cascade of neural events that fundamentally reorganises how the brain processes information.
But here’s the key to understanding why LSD lasts so long: when an LSD molecule lands on a 5-HT2A serotonin receptor, the receptor physically folds over the molecule and locks it in place — like a trapdoor closing. The drug’s effects will not begin to fade until the molecules are knocked off or come loose from the receptor. This can take anywhere from 6 to 15 hours. The brain essentially traps its own disruptor inside its own machinery, and cannot stop the experience until the molecule works its way free on its own terms.
Additionally, LSD has recently been found to act as a highly potent positive allosteric modulator of TrkB — the receptor for Brain-Derived Neurotrophic Factor (BDNF) — which explains why even a single LSD experience can produce measurable neuroplastic changes that persist for weeks or months after the molecule itself is completely gone.
Neuroimaging studies, most importantly the landmark 2016 work from Imperial College London’s Centre for Psychedelic Research, confirm that LSD reduces the efficacy of thalamo-cortical information filtering, decreases oscillatory power within the default mode network, and fundamentally flattens the hierarchical organisation of large-scale brain activity. What this means in experiential terms unfolds over the following hours.
The Hour-by-Hour Brain Breakdown
Note: The timeline below is based on a standard oral dose of approximately 100–150 micrograms of LSD, taken on an empty stomach. Individual experiences vary based on dose, body weight, metabolism, emotional state, and environment.
⏱ Minutes 0–30: Ingestion and the Invisible Beginning
The tab goes under the tongue. The clock starts. And for the first twenty to thirty minutes: nothing you can consciously detect.
But things are already moving. LSD is being absorbed through the sublingual mucosa into the bloodstream. It passes through your stomach and small intestine, enters the bloodstream, and is carried through the body and into the brain. Your liver begins metabolising it using the CYP2D6 enzyme — but this process is slow, and most of the active compound reaches the brain intact.
Pharmacokinetic data from a landmark 2017 clinical study at the University of Basel found that in healthy subjects given a 200 microgram oral dose, mean maximal LSD plasma concentrations were reached at a median of 1.5 hours post-administration — but the compound begins crossing the blood-brain barrier and binding to receptors well before plasma levels peak. The average duration of subjective effects ranges from 6.7 hours at the lowest doses to 11 hours at higher doses.
At this moment in the timeline, your neurons are beginning their encounter with LSD molecules for the first time. 5-HT2A receptors in the prefrontal cortex begin to activate. The thalamus — the brain’s gatekeeper and sensory relay station — begins receiving altered signals. Nothing is visible yet. But the machinery is turning.
What you feel: A quiet awareness that something is different. Perhaps a faint electric quality to the air. A subtle luminosity to colours. A restlessness or excitement that is hard to source. Some people feel mild nausea or stomach awareness during this window, particularly on a full stomach.
What your brain is doing: LSD molecules are landing on 5-HT2A receptors and being locked in place. The prefrontal cortex is beginning to receive dramatically altered serotonergic input. The thalamic gating mechanism — which normally filters the overwhelming torrent of raw sensory data before it reaches conscious awareness — is beginning to loosen.
⏱ Hour 1: The Come-Up — Reality Softens
This is when you know. Unambiguously, undeniably, irreversibly: you know.
The come-up of LSD is distinct — and for many people, it is one of the most electrically charged hours of the entire experience. The world begins to reorganise. Colors become saturated in a way that seems impossible — not brighter exactly, but more present, as if the visual filter you’ve always lived behind has been partially removed. Surfaces begin to breathe. Objects acquire subtle movement and texture they didn’t have before.
The thalamic filter is failing. Under normal circumstances, the thalamus — acting as the brain’s “information gatekeeper” — filters the massive raw stream of sensory data flowing in from your eyes, ears, skin, and internal organs, and passes only what it deems relevant to conscious awareness. LSD disrupts this filtering. Suddenly, more of everything gets through. The world doesn’t look different because your eyes are seeing differently — it looks different because your brain is letting you see more of what was always there.
At the neurological level, the serotonin 5-HT2A receptors in the visual cortex are now significantly activated. Research from Imperial College London’s landmark 2016 neuroimaging study, published in the Proceedings of the National Academy of Sciences, showed that increased visual cortex cerebral blood flow and dramatically expanded primary visual cortex (V1) functional connectivity correlated strongly with ratings of visual hallucinations — implying that intrinsic brain activity exerts greater influence on visual processing in the psychedelic state. The visual system is no longer passively receiving the outside world. It has become an active generator of experience.
Emotional effects intensify. LSD can amplify your mood significantly. If you’re in a positive, safe environment when the come-up hits, you may feel waves of warmth, joy, and profound gratitude for existence. The emotional tone of the come-up is one of the strongest predictors of the trip’s overall character — which is why “set and setting” (your mental state and environment) matters so profoundly at this moment. If anxiety or fear is present, this hour can feel destabilising.
Time begins to distort. Nearly all people who take LSD report that it alters their perception of time. During the come-up, time typically slows and thickens — what feels like an hour may be twenty minutes. Your relationship to clock time begins its long departure.
Physical effects emerge: Pupil dilation (one of LSD’s most reliable physical signatures). Slight elevation in blood pressure and heart rate. Mild jaw tension. A tingling or electric sensation across the skin. Body temperature fluctuation — waves of warmth followed by subtle chills. These are largely the result of LSD’s secondary activity at adrenergic receptors, producing a mild sympathomimetic response.
What to do: This is the moment to be where you want to be. Find a safe, comfortable space. Don’t fight the come-up — it cannot be stopped, and resistance amplifies anxiety. Breathe slowly. Trust that what is coming is temporary.
⏱ Hours 2–3: The Brain’s Normal Organisation Dissolves
By the second hour, LSD is doing something that no other pharmacological event in ordinary life produces. It is dismantling the default architecture of your brain.
Under normal circumstances, the brain operates through segregated, specialised networks. The visual network handles vision. The auditory network handles sound. The default mode network manages self-referential thought, memory, and the sense of being a distinct “you.” These networks operate relatively independently — each doing its job without excessive cross-communication.
LSD terminates this arrangement.
Research published in Current Biology from Imperial College London, titled Increased Global Functional Connectivity Correlates with LSD-Induced Ego Dissolution, demonstrated that LSD dramatically increases global functional connectivity across the brain — networks that normally operate independently begin communicating with each other extensively. The visual network starts receiving input from the auditory network. The emotional processing regions begin feeding into sensory cortex. The default mode network loses its coherence and its grip on the self.
And from a Nature Communications study using network control theory and fMRI data: LSD and psilocybin flatten the brain’s control energy landscape, reducing the energetic cost of transitioning between brain states. Where the normal brain follows constrained neural highways — predictable paths from state to state — the LSD brain becomes a landscape where those highways have dissolved and every direction is equally navigable. Brain state transitions become fluid, effortless, and radically unpredictable.
Synesthesia begins. When network segregation breaks down, the senses begin bleeding into each other. Music becomes visual — you may see sounds as colours, shapes, or spatial forms. Textures may have tastes. Light may have sound. This is real synesthesia — not metaphor — produced by the literal cross-activation of sensory cortices that do not normally communicate. It is one of LSD’s most reliably reported and scientifically documented phenomena.
Thought patterns accelerate and liquefy. Ideas connect to other ideas with unusual speed and emotional resonance. Conceptual leaps that would ordinarily require deliberate analytical effort happen spontaneously and feel profoundly meaningful. This is the “entropic brain” — the term coined by neuroscientist Robin Carhart-Harris to describe the state of increased neural entropy produced by psychedelics, in which the brain’s spontaneous activity becomes more complex, more diverse, and less constrained by its usual hierarchical order.
The ego begins to loosen. The default mode network — the brain’s self-referential hub, responsible for your internal narrative, your sense of being a distinct person separate from the world — is losing its coherent grip. You may begin to notice that the internal voice that usually narrates your experience is quieting. This is the beginning of what will deepen, at higher doses, into full ego dissolution.
⏱ Hours 3–5: The Peak — The Brain Rebuilt From Scratch
The peak of an LSD trip at a standard dose typically occurs between 2 and 4 hours after ingestion, with the most intense effects lasting through the fifth hour. This is the deepest territory of the experience, and the most scientifically documented.
Here is what is concurrently happening in the brain during the LSD peak:
The visual cortex is generating reality, not receiving it. Imperial College’s neuroimaging research showed that under LSD with eyes closed, many more areas of the brain than normal contribute to visual experience. The closed-eye visuals of LSD — geometric mandalas, fractal architectures, landscapes of impossible colour and depth — are not random static. They are the brain’s own imagery, generated internally, now amplified and projected with the same perceptual conviction as ordinary reality. As Dr. Robin Carhart-Harris described: “We observed brain changes under LSD that suggested our volunteers were ‘seeing with their eyes shut’ — albeit they were seeing things from their imagination rather than from the outside world.”
Ego dissolution reaches its fullest expression. At peak, the default mode network has lost its normal dominance. Research from Imperial College London published in PNAS showed that decreased connectivity between the parahippocampus and retrosplenial cortex correlated strongly with ratings of “ego dissolution” and “altered meaning” — implying the importance of this particular circuit for the maintenance of “self” and its processing of “meaning.” When this circuit loses coherence, the subjective experience is a dissolution of the boundary between self and world. The internal narrator quiets or disappears. There is awareness, but it is no longer owned by anyone. Many people describe this as one of the most profound experiences of their lives. It is also, for some people, the most frightening.
A 2025 study from King’s College London and Imperial College London, published in Human Brain Mapping, specifically identified the dorsolateral prefrontal cortex (DLPFC) and its connection to the thalamus as critical nodes in the “ego dissolution network” — finding that LSD increased information flow between these regions in the theta band, substantiating the hypothesis that disruptions in thalamic gating underlie the experience of ego dissolution. The thalamus — which normally acts as the gatekeeper between raw experience and conscious awareness — has become permeable, allowing what was previously filtered to flood into consciousness.
Emotional intensity reaches its maximum. The peak of LSD amplifies whatever emotional material exists in the psyche at that moment. Joy becomes ecstasy. Wonder becomes awe. Fear becomes terror. Love becomes a cosmic force. The limbic system — the brain’s emotional processing hub — is receiving maximally disrupted input from a prefrontal cortex that can no longer apply its usual regulatory brakes. Emotional material that normally sits beneath the surface of awareness can emerge with startling power and clarity.
The REBUS model — what this all means. The dominant scientific model for how LSD and other psychedelics alter consciousness is the REBUS model — Relaxed Beliefs Under Psychedelics — developed by Carhart-Harris and colleagues. It proposes that psychedelics alter conscious experience by relaxing the brain’s top-down “prior beliefs” about how the world should be perceived, and allowing bottom-up sensory information to exert greater influence on experience. The predictive processing machine that normally constructs a stable, reliable, consensus reality from raw sensory data has been partially disabled. What replaces it is an experience built more directly from raw perception — which is simultaneously more vivid, more meaningful, more emotionally resonant, and far less predictable.
Time has stopped making sense. At peak, objective clock time becomes genuinely irrelevant. Many users report that peak states felt like hours when only minutes passed, or that entire lifetimes seemed to be experienced in a single moment. This is not subjective impression — it reflects real changes in the brain’s temporal processing. The normal rhythmic oscillations that help the brain track time have been disrupted by LSD’s action on multiple receptor systems.
⏱ Hours 5–7: The Plateau — Integration Begins
After the peak, the intensity begins to soften — but only gradually, and not linearly. LSD’s plateau phase is long: the effects remain significantly active for two to three hours after the peak, gradually declining in intensity while remaining qualitatively similar in character.
Visual phenomena remain present but become more gentle. Open-eye visuals — the breathing of surfaces, the movement of patterns, the unusual saturation of colour — continue but are less overwhelming. Closed-eye visuals soften from architectural complexity to flowing imagery. The sense of ego dissolution typically relaxes into something more like profound openness or expanded awareness — still distinctly psychedelic, but no longer boundless.
Cognitively, the plateau is often where the most meaningful personal material surfaces. With the peak’s overwhelming intensity behind you, the mind begins to process what it has encountered. Insights — about your life, your relationships, your patterns, your fears, your purpose — arise with unusual clarity and felt certainty. These insights are not random. They reflect the brain’s enhanced connectivity and reduced self-referential defensiveness, which together create conditions in which emotional and psychological material can be seen without the usual distortions of ego-protection.
Music takes on particular significance during this phase. Research from the Beckley/Imperial Research Programme found that listening to music while on LSD triggered significant changes in how the brain processes and integrates auditory information — with emotional responses to music substantially amplified, and the subjective meaning of musical pieces dramatically enhanced. Many people describe specific pieces of music heard during an LSD plateau as among the most moving and meaningful musical experiences of their lives.
Physically, the body is still in sympathomimetic activation — elevated heart rate, pupil dilation, muscle tension. Fatigue begins to accumulate beneath the experience, as the nervous system has been running at elevated capacity for hours. Staying hydrated and warm is important during this window.
⏱ Hours 7–9: The Descent — Reality Re-Assembles
The brain’s default networks begin to reassert themselves. The 5-HT2A receptors, still occupied by LSD molecules, are beginning to release them gradually as the molecules come loose from their receptor pockets under the body’s metabolic pressure.
Visual distortions continue to fade. Open-eye movement and colour saturation diminish. The internal narrative — the self, the ego, the “I” — gradually returns. This return is often accompanied by a profound sense of relief and, simultaneously, a particular kind of wistfulness — the recognition that something enormous is receding.
After the peak of an LSD trip, the comedown signals the gradual return to normal consciousness, with LSD’s effects slowly fading. Hallucinations start fading, but thoughts may remain abstract and introspective. Some experience mental and physical exhaustion from the intensity of the peak phase, while many describe the late descent as peaceful, with a sense of profound clarity and emotional settledness.
Cognitively, this is a valuable window. The brain remains more plastic and less defensively organised than in ordinary waking life, but is no longer overwhelmed. Insights from earlier in the experience can be examined, turned over, and articulated — often for the first time. This is an excellent time to write, if you have the energy and focus.
Some people experience mild anxiety during the descent — a sense of returning to ordinary reality that feels, after the expanse of the peak, somewhat constraining. This is normal and passes. The brain is literally rebuilding the structures of ordinary consciousness, and the process isn’t always seamless.
⏱ Hours 9–12: The Comedown — Reintegration
By this stage, most of the drug’s acute psychedelic effects have subsided. The visual field has returned to normal. The ego is back. Time flows normally again. The trip is over in its most dramatic sense — but the experience is not finished.
What remains in the comedown is a particular quality of consciousness that is hard to describe to anyone who hasn’t experienced it: a profound emotional tenderness, a heightened perceptual sensitivity, and a feeling of having travelled somewhere enormous and returned changed. Simple things — a glass of water, a conversation with a friend, the texture of a blanket — can feel unusually meaningful and present.
Physically, the body is tired. The sympathomimetic activation of the past several hours has been energetically costly, and fatigue now asserts itself clearly. Muscle tension, mild headache, jaw soreness, and physical heaviness are common. This is not toxicity — it’s the ordinary exhaustion of a nervous system that has been running at extraordinary intensity for most of a day.
Sleep is typically difficult during the comedown phase. Even when the acute effects have faded, the brain remains subtly activated — more associative, less prone to the settled, downregulated state that supports sleep. Most people find they cannot sleep until 10 to 14 hours after ingestion, even if the trip itself ended earlier.
Emotionally, the comedown is highly variable. Many people feel a deep, settled peace — a sense of having processed something significant and having arrived somewhere new. Some feel fragile and tender, which is equally valid. Some feel mild flat affect or low mood as the dopamine and serotonin systems recalibrate to baseline. All of these responses are normal and temporary.
⏱ Hours 12–24: The Afterglow — Something Remains
The afterglow of LSD is real, documented, and one of the most therapeutically significant aspects of the experience.
After your trip is over, you may experience “afterglow” effects for another six hours — lingering effects of happiness, emotional openness, or a feeling of “lightness” in life. Between the initial trip and the comedown, it can take up to 24 hours for your body and brain to return fully to their typical state.
The afterglow is characterised by heightened emotional sensitivity, enhanced perspective, unusual clarity about what matters in life, and a sense of connection to others and to the world that carries a particular quality of realness and intimacy. It is not a residue of the psychedelic state — it is the brain’s newly reorganised neural architecture experiencing the ordinary world through eyes that have been fundamentally changed.
Research published in Psychopharmacology on long-lasting subjective effects of LSD in healthy subjects found that after a single 200 microgram dose, positive attitudes about life and self, positive mood changes, altruistic and positive social effects, and positive behavioral changes were all significantly elevated — not just immediately after, but at 1 month and 12 months follow-up. After 12 months, 10 of 14 participants rated their LSD experience as among the top 10 most meaningful experiences of their entire lives.
The afterglow is also when the most important integration work begins. The neurological “writing window” is open — the brain is in a state of heightened plasticity, and what you think, feel, and reflect on during this period will shape what new patterns consolidate. Journaling, reflective conversation, time in nature, and gentle creative work are all excellent uses of the afterglow.
What LSD Does to the Brain: A Neuroscience Summary
1. The 5-HT2A Receptor Is the Master Switch
All of LSD’s primary psychedelic effects — the visual hallucinations, the ego dissolution, the enhanced emotional intensity, the time distortion — are mediated through the 5-HT2A serotonin receptor. Research from multiple institutions has confirmed that blocking this receptor with ketanserin (a 5-HT2A antagonist) completely prevents the psychedelic response to LSD, even at high doses. The 5-HT2A receptor is most densely expressed in the higher-order cortical regions responsible for self-referential thought, sensory integration, and executive function — exactly the regions that LSD’s experience most profoundly disrupts.
2. The Default Mode Network Goes Offline
The Default Mode Network (DMN) — the brain system responsible for self-referential thought, internal narrative, and the sense of being a distinct “self” — is significantly suppressed by LSD. Neuroimaging studies consistently show decreased DMN connectivity and oscillatory power under LSD, which correlates directly with the subjective experience of ego dissolution. When the DMN loses its grip, the experience of being a bounded, separate self dissolves — and what remains is awareness without a defined centre.
3. Global Brain Connectivity Explodes
LSD dramatically increases global functional connectivity — the degree to which distinct brain networks communicate with each other. Under normal conditions, brain networks are segregated: each does its own job. Under LSD, this segregation breaks down and a state of massively increased global communication emerges. This is what produces synesthesia, the sense of universal connection, the perception that everything is deeply interrelated, and the dreamlike quality of LSD’s visual and conceptual content.
4. The Brain’s Energy Landscape Flattens
Research using network control theory published in Nature Communications demonstrated that LSD flattens the brain’s “control energy landscape” — reducing the energetic cost required to transition between brain states. Under normal conditions, the brain follows well-worn neural pathways, transitioning between states with specific energetic requirements. LSD makes all state transitions equally easy, producing an experience of radical psychological fluidity — the mind moves freely between emotional registers, conceptual frameworks, and perceptual modes without the usual friction of ordinary consciousness.
5. Neuroplasticity Is Promoted
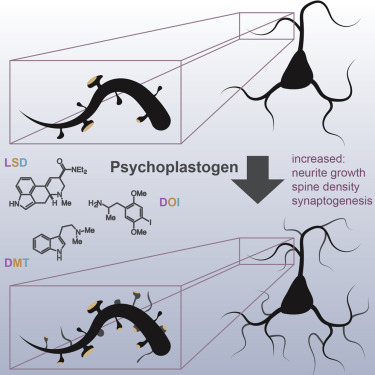
LSD, like other psychedelic compounds, has been found to increase the expression of genes related to synaptic plasticity — what researchers call “psychoplastogenic effects.” This appears to be mediated by serotonin 5-HT2A receptor agonism and by LSD’s action as a potent positive allosteric modulator of TrkB, the BDNF receptor. Research from Ly et al. (2018) showed that LSD, DMT, and related compounds significantly increase the complexity of dendritic arbours and promote neuritogenesis and spinogenesis — the physical growth of new neural connections. The experience of LSD is not just a pharmacological event. It is a neuroplastic one.
LSD vs Psilocybin: The Key Differences
The most common question people have about LSD is how it compares to magic mushrooms. Both are serotonergic psychedelics acting primarily at 5-HT2A receptors, and both produce broadly similar neurological effects — ego dissolution, increased global connectivity, suppressed DMN activity. But there are important differences worth understanding:
Duration: LSD lasts significantly longer — typically 8–12 hours vs. 4–6 hours for psilocybin. This makes LSD a more demanding commitment in both preparation and integration.
Character: LSD is generally described as more stimulating, more visually precise, and more cognitively activating. Psilocybin tends to feel warmer, more emotional, and more inwardly directed. This is likely due to LSD’s additional activity at dopaminergic and adrenergic receptors, which psilocybin lacks.
Dose control: Psilocybin mushrooms offer more transparent dosing — you can measure grams of dried mushroom with reasonable predictability. LSD doses on blotter paper are impossible to verify without chemical testing, which adds significant harm-reduction complexity.
Onset: LSD has a longer, more gradual come-up than psilocybin — which can feel more abrupt and wave-like in its onset.
LSD is not just being studied as a curiosity. It is being actively investigated as a treatment for some of the most treatment-resistant conditions in modern psychiatry.
LSD is currently being explored in conjunction with psychological support as a treatment for generalized anxiety disorder and depression, with research ongoing at Imperial College London and other institutions. A 2025 study from King’s College London specifically investigated LSD’s role in ego dissolution as it relates to depression — noting that hypofunction in the left dorsolateral prefrontal cortex is associated with depression, and that LSD’s action on this region may be one mechanism of its antidepressant potential.
The clinical picture at this stage is promising but early. What is established is that a single high-dose LSD experience, when properly supported, can produce lasting positive changes in personality, mood, and life satisfaction that persist for twelve months or longer. That’s not a drug effect — that’s a transformation.
Harm Reduction: What You Need to Know
✅ Essential Prerequisites
No personal or family history of psychosis, schizophrenia, or bipolar disorder
Not currently on SSRIs, MAOIs, or lithium — these can interact unpredictably and dangerously with LSD
A trusted, sober companion present — particularly important for first experiences or higher doses
A safe, private, comfortable physical environment
Clear intention set in advance
An integration plan for the days following the experience
✅ Dose Awareness
For most people, a dose of 1 to 3 micrograms per kilogram of body weight is enough to produce a moderate trip. If you haven’t used LSD before, starting with a smaller dose is important — and without chemical testing, it’s impossible to know exactly how much LSD is in any product you choose to take. Reagent testing kits (Ehrlich test) can confirm the presence of an indole compound but cannot determine dose.
✅ Set and Setting
Your mindset and your environment are the two most powerful determinants of whether an LSD experience is positive or difficult. Your current mood and emotional state are amplified dramatically by LSD — if significant anxiety, unresolved grief, or interpersonal conflict is present going in, it will likely surface during the trip. Choose your environment, your company, and your day carefully.
✅ If Things Get Difficult
The primary tool for a difficult LSD experience is surrender rather than resistance. Resisting a difficult psychedelic experience amplifies it. Accepting it — moving toward it rather than away from it — tends to allow it to pass. The key harm-reduction reminder: no one has ever died from a normal LSD experience. Whatever you are experiencing is temporary. The molecule will come loose from its receptor binding and the experience will end.
✅ Integration Is Non-Negotiable
The 24–72 hours following an LSD experience are a critical window for integration. Journal. Sleep. Move your body. Speak with a trusted friend or therapist about what emerged. For our complete guide to psychedelic integration, read our Integration Guide.
Frequently Asked Questions
Why does LSD last so much longer than mushrooms?
The primary reason is LSD’s unique receptor binding mechanism. When LSD molecules land on 5-HT2A receptors, the receptor physically closes over the molecule, trapping it in place. The experience continues until those molecules work free on their own — which can take 6 to 15 hours. Psilocin (the active metabolite of psilocybin) does not bind with the same locked persistence, which is why mushroom trips typically last 4–6 hours.
What actually causes visual hallucinations on LSD?
Neuroimaging research from Imperial College London showed that under LSD, increased blood flow to the visual cortex and dramatically expanded primary visual cortex (V1) functional connectivity correlate strongly with visual hallucinations. The brain’s intrinsic visual activity — normally suppressed by top-down filtering — breaks through into conscious awareness. The visuals are generated by the brain itself, not by external stimuli. The eyes are just the canvas.
Is ego dissolution dangerous?
Ego dissolution is not dangerous in the sense of causing brain damage or physical harm. It can be profoundly disorienting, and for some people it is frightening. For others it is described as the most profound and positive experience of their lives. The experience of ego dissolution appears to be associated with lasting improvements in well-being, openness, and life satisfaction in clinical research. The critical factor is preparation, context, and the presence of a trusted sitter if the experience becomes overwhelming.
Does LSD cause permanent brain damage?
There is no credible scientific evidence that LSD at normal doses causes permanent brain damage. LSD is considered non-toxic at standard doses, and death from LSD alone is extremely rare. The primary risks are psychological — bad trips, HPPD (hallucinogen persisting perception disorder, which occurs in a small minority of users), and triggering of latent psychiatric conditions in those predisposed. These risks are real and worth taking seriously, but they are not the same as structural brain damage.
How is LSD different from a bad trip?
A “bad trip” is not a different chemical event — it’s the same neurological experience with a different emotional and psychological content. The amplification of emotion, dissolution of ego, and loss of ordinary perceptual filters are identical. What differs is the material that surfaces, the person’s relationship to it, and their capacity to surrender to the experience rather than resist it. A challenging LSD experience can be among the most therapeutically meaningful — when approached with the right tools, support, and integration framework.
The Bottom Line
Buy LSD Online in Canada!
Your brain on LSD is not broken. It is not malfunctioning. It is operating at maximum capacity with its normal constraints temporarily removed.
For twelve hours, the brain’s usual hierarchical order — the filtering, the categorising, the protecting, the self-narrating — is dramatically relaxed. What floods in is raw experience: more sensory, more emotional, more connected, more present, and simultaneously more uncertain and more real than ordinary consciousness typically allows.
The neuroscience of this process is among the most fascinating in modern medicine. The 5-HT2A receptors locking LSD in place. The thalamic gatekeeper failing to filter. The default mode network losing its grip on the self. The global brain connectivity exploding. The control energy landscape flattening into radical freedom of state.
And then, slowly, over twelve hours, reality reassembles — but not quite the way it was before. Because the brain that comes out the other side is not the same brain that went in. New connections have been built. Old patterns have been interrupted. Something has been seen that cannot be unseen.
That, hour by hour, is what happens to your brain on LSD.
Curious about exploring psychedelics safely and intentionally? Browse our full selection of magic mushrooms, or read our complete Microdosing 101 Guide to start smaller and more gently.
Sources
Carhart-Harris, R.L. et al. (2016) — “Neural correlates of the LSD experience revealed by multimodal neuroimaging” — PNAS — https://pubmed.ncbi.nlm.nih.gov/27071089/
Tagliazucchi, E. et al. (2016) — “Increased Global Functional Connectivity Correlates with LSD-Induced Ego Dissolution” — Current Biology — https://pubmed.ncbi.nlm.nih.gov/27085214/
Schmid, Y. et al. (2021) — “Acute dose-dependent effects of lysergic acid diethylamide in a double-blind placebo-controlled study in healthy subjects” — PMC — https://pmc.ncbi.nlm.nih.gov/articles/PMC8027607/
Suárez-Pinilla, M. et al. (2025) — “The Role of the Dorsolateral Prefrontal Cortex in Ego Dissolution and Emotional Arousal During the Psychedelic State” — Human Brain Mapping — https://pmc.ncbi.nlm.nih.gov/articles/PMC11979361/
Singleton, S.P. et al. (2022) — “Receptor-informed network control theory links LSD and psilocybin to a flattening of the brain’s control energy landscape” — Nature Communications — https://www.nature.com/articles/s41467-022-33578-1
Carhart-Harris, R.L. & Friston, K.J. (2019) — “REBUS and the Anarchic Brain: Toward a Unified Model of the Brain Action of Psychedelics” — Pharmacological Reviews
Ly, C. et al. (2018) — “Psychedelics promote structural and functional neural plasticity” — Cell Reports
Disclaimer: This blog is for educational and harm reduction purposes only and is not medical advice. LSD is a controlled substance in many jurisdictions. Always research the laws in your area before proceeding.
If you’ve spent any time in the microdosing world, you’ve almost certainly heard the name Paul Stamets. And if you’ve heard his name, you’ve almost certainly heard about the Stack.
The Stamets Protocol — a specific combination of psilocybin, Lion’s Mane mushroom, and niacin — has become one of the most talked-about, debated, and widely practiced microdosing regimens in the world. Silicon Valley professionals microdose it for cognitive edge. Depression sufferers use it as a therapeutic bridge. Neuroscience enthusiasts follow it for its neuroplasticity potential. And thousands of ordinary people use it simply because they heard Paul Stamets describe it on a podcast and couldn’t stop thinking about it.
But what exactly is the Stamets Stack? What does each ingredient actually do? How does the combination work? And most importantly — what does the science actually say?
This blog breaks it all down. No hype, no oversimplification — just a clear, honest look at one of the most interesting neurochemical experiments happening in kitchens and capsule makers around the world right now.
Who Is Paul Stamets?
Before we get into the Stack itself, it helps to understand who developed it and why.
Paul Stamets is one of the most decorated and prolific mycologists alive today. Author of six books on mushrooms including the landmark Psilocybin Mushrooms of the World, Stamets has spent decades studying the medicinal, ecological, and neurological potential of fungi. He holds over 20 mushroom-focused patents. He starred in the documentary Fantastic Fungi. He runs Fungi Perfecti, one of the most respected medicinal mushroom companies in North America. And he has dedicated the latter part of his career to advocating for the responsible scientific investigation of psilocybin.
Stamets introduced the idea of stacking psilocybin, lion’s mane, and niacin as a way to promote what he calls “epigenetic neurogenesis” — suggesting that the combination could help the brain grow new cells and pathways. He was motivated significantly by the alarming rise of neurodegenerative conditions like Alzheimer’s disease.
In 2018, Stamets filed a formal patent application with the U.S. Patent and Trademark Office for a composition combining psilocybin or psilocin with erinacines or hericenones (Lion’s Mane bioactives) and niacin — claiming it as a unique method for enhancing neuroregeneration and cognition. The patent describes methods for “enhancing neurogenesis, resolving neuropathy and improving neurological health and functioning” using this combination.
That’s the origin story. Now let’s get into the science of each ingredient.
Ingredient #1 — Psilocybin: The Neuroplasticity Catalyst
Psilocybin is the star of the Stack. In the Stamets Protocol, it’s used at microdose levels — sub-perceptual amounts that produce no psychedelic effects whatsoever, but appear to produce meaningful neurological changes.
A standard microdose of psilocybin in the Stamets Stack is approximately 0.1 to 0.3 grams of dried Psilocybe cubensis — roughly 1/10th to 1/20th of a recreational dose. At these levels, you won’t experience visual distortion, ego dissolution, or any significant alteration of consciousness. What you may notice is a subtle lift in mood, a slight sharpening of focus, and a feeling of mental flexibility that’s hard to precisely describe but consistently reported.
At the pharmacological level, psilocybin is converted in the body to psilocin, which binds to serotonin 2A receptors (5-HT2A) in the prefrontal cortex. At microdose levels, this activation is gentle — but it’s still triggering the same fundamental neuroplasticity cascade that makes high-dose psilocybin so remarkable.
Specifically, psilocybin at even sub-perceptual doses is believed to encourage neuroplasticity — the brain’s ability to reorganize and form new neural connections. Research from Yale University published in Neuron in 2021 showed that a single dose of psilocybin produced approximately a 10% increase in dendritic spine density in the frontal cortex of mice — new physical connections between neurons — that persisted for at least a month. That’s the structural change Stamets is trying to support chronically and gently with the microdosing protocol.
Stamets also theorized specifically that psilocybin at low doses creates a “window” of enhanced neuroplasticity — and that this window is when Lion’s Mane’s nerve growth factors can most effectively build and reinforce new neural structures. Psilocybin opens the door; Lion’s Mane walks through it.
Lion’s Mane (Hericium erinaceus) is the non-psychedelic powerhouse of the Stack — and the ingredient that most clearly complements psilocybin’s effects at a molecular level.
Lion’s Mane is a shaggy, tooth-like fungus that has been used in traditional Chinese medicine for centuries and naturally grows in North America, Europe, and Asia. What makes it remarkable from a neuroscience perspective is its unique bioactive compounds: hericenones (found in the fruiting body) and erinacines (found in the mycelium). Both classes of compounds have been shown in preclinical research to stimulate the production of Nerve Growth Factor (NGF).
NGF is a protein that supports the survival, growth, and maintenance of nerve cells — essentially biological fertilizer for your neurons. It promotes the formation of new neural connections, supports the health of existing ones, and plays a critical role in the maintenance of the basal forebrain cholinergic system — the brain region most devastated by Alzheimer’s disease.
Research published in PubMed confirmed that hericenones and erinacines isolated from Lion’s Mane can induce NGF synthesis in nerve cells. Crucially, both hericenones and erinacines can easily cross the blood-brain barrier — which means they don’t just circulate in the bloodstream but actively reach and act on brain tissue.
Multiple studies have examined Lion’s Mane’s clinical effects:
A 2009 double-blind clinical trial showed improvements in mild cognitive impairment in adults aged 50–80 after 16 weeks of Lion’s Mane supplementation. The improvements were observed throughout the trial but not at the follow-up 4 weeks after cessation — suggesting prolonged supplementation is necessary to maintain benefits.
Animal studies have shown that Lion’s Mane extract reduces anxiety and depressive behaviors by promoting hippocampal neurogenesis in the adult mouse brain.
A 2023 study in the Journal of Neurochemistry found that hericerin derivatives from Lion’s Mane activate a pan-neurotrophic pathway in central hippocampal neurons, converging to ERK1/2 signaling and enhancing spatial memory.
Erinacine A, one of the most studied compounds from Lion’s Mane mycelium, has been shown in multiple animal models to reduce amyloid-beta deposition associated with Alzheimer’s disease, and in a 49-week human trial to produce improvements in Mini-Mental State Examination scores in patients with mild Alzheimer’s.
Stamets has specifically called Lion’s Mane the “second smart mushroom,” emphasizing that it “reinforces psilocybin’s ability to occasion neurogenesis.” The rationale is elegant: psilocybin creates the neuroplastic conditions for new neural growth, while Lion’s Mane provides the NGF that fuels that growth and gives it structural support.
By including Lion’s Mane in the stack, Stamets aimed to provide the brain with building blocks for regeneration and cognitive enhancement — not just creating neuroplasticity, but filling it with meaningful biological material.
Of the three ingredients, niacin is the one that raises the most eyebrows. It’s a B vitamin. Why is a B vitamin in a neurogenesis stack?
This is where Stamets’ thinking gets genuinely creative.
Niacin (Vitamin B3), specifically in its flushing form — nicotinic acid — causes a phenomenon called the niacin flush when taken at doses of 50mg or higher. This flush is a prickly, warm, reddening sensation caused by the release of prostaglandins that widen blood vessels and dilate capillaries throughout the body. Within 15–20 minutes of taking niacin, blood flow to the skin and peripheral tissues surges noticeably.
Stamets’ hypothesis is that this vasodilation does something critically important: it drives the active compounds of both psilocybin and Lion’s Mane to the far reaches of the nervous system — to the nerve endings in the peripheral nervous system where, according to Stamets, the majority of neurogenesis actually occurs. Stamets reports that niacin works as a flushing agent and carries compounds across the blood-brain barrier, helping to distribute the psilocybin and Lion’s Mane deeper into the brain and nervous system, enhancing their healing potential.
Stamets also notes that psilocybin tends to mildly constrict blood vessels, while niacin dilates them — making niacin a pharmacological counterbalance that potentially improves the bioavailability and distribution of psilocin throughout the nervous system.
Importantly, Stamets specifies using flushing niacin (nicotinic acid) — not the “no-flush” form sold as niacinamide. The flush is not a side effect to be avoided. It is the mechanism. Non-flushing versions of vitamin B3 do not offer the same delivery benefits and are not part of this protocol.
Beyond its delivery role, niacin has independently documented brain health benefits. One large epidemiological study found that higher dietary niacin intake was associated with a lower risk of Alzheimer’s disease and age-related cognitive decline. Niacin is also essential for cellular energy metabolism as a precursor to NAD⁺, plays a role in DNA repair and cell signalling, and has anti-inflammatory properties.
Stamets has also noted a clever harm-reduction feature built into niacin’s inclusion: the flush acts as a deterrent to high-dose misuse. If someone attempts to take a full psychedelic dose alongside a high niacin dose, the intense, uncomfortable flush — deep redness, itching, and burning sensation — will make that experience deeply unpleasant and discourage repetition. The niacin acts, in his words, as a built-in “anti-abuse” mechanism.
The Synergy: Why Three Is Greater Than One
The power of the Stamets Stack lies not in each ingredient individually — but in the theorized interaction between all three. Here’s how Stamets envisions they work together:
Psilocybin — at microdose levels — binds to 5-HT2A receptors in the prefrontal cortex, triggering a cascade of neuroplastic changes. New dendritic spines begin forming. The brain enters an enhanced state of structural flexibility.
Lion’s Mane simultaneously floods the brain with hericenones and erinacines — compounds that stimulate NGF and BDNF production. These growth factors provide the biological “materials” needed to build new neural connections. The psilocybin-induced neuroplasticity window gives those growth factors more surface area to work with.
Niacin opens the circulation highways, driving both sets of compounds deeper into the nervous system — particularly to the peripheral nerve endings where Stamets believes neuroregeneration is most needed and where the compounds might otherwise struggle to penetrate.
In his own words from the patent application: “psilocin and its analogs are neurotransmitters, and substitute for serotonin, acting as an agonist exciting serotonin receptors, their ability to enhance neurotransmission while in combination with nerve growth factors such as erinacines and hericenones, provides a unique opportunity for spurring neurogenesis. When combined with niacin, which causes nerve ending excitement, and additionally combined with mushroom and plant extracts, compounded neurogenic benefits are anticipated.”
In short, the theory is: psilocybin opens the window, Lion’s Mane builds through it, and niacin makes sure delivery reaches the furthest corners of the house.
What Does the Science Actually Say?
This is the question that separates enthusiasts from researchers — and the honest answer is: promising but not yet proven.
Here’s what we actually know:
On psilocybin alone: The neuroplasticity evidence is robust and growing. The 2021 Yale study on dendritic spine density, the 2025 Cornell study on psilocybin rewiring entire brain networks, and multiple human clinical trials at Johns Hopkins confirm that psilocybin produces real, measurable, lasting structural brain changes. The evidence for psilocybin’s neuroplasticity effects — even at low doses — is the strongest leg of the Stack.
On Lion’s Mane alone: The preclinical evidence (primarily in cell cultures and animal models) for NGF stimulation via hericenones and erinacines is well-established. Human clinical data is more limited but encouraging — particularly the 2009 cognitive impairment trial and emerging Alzheimer’s research. A 2022 observational study published in Nature Scientific Reports found that microdosers using psilocybin combined with Lion’s Mane and niacin reported better mental health outcomes than those microdosing psilocybin alone.
On the full Stack: This is where the evidence gap becomes clear. The full synergistic combination — all three components together — has not yet been the subject of a robust, placebo-controlled human clinical trial. A large 2022 observational study of nearly 1,000 microdosers found that those using the Stamets Stack reported better mental health outcomes than psilocybin-only microdosers, and critically, adults over 55 who used the full Stack exhibited greater improvements in psychomotor performance compared to psilocybin alone.
However, the researchers correctly acknowledged that this was observational, self-reported data. The improvements could reflect expectancy effects (placebo), reporting bias, or genuine pharmacological synergy — it’s not possible to distinguish between them without a controlled trial.
The honest scientific assessment: each ingredient has individual evidence, a promising observational signal exists for the combination, and rigorous controlled trials are the next necessary step. Stamets himself has co-founded MycoMedica Life Sciences, which has raised $60 million and is working toward exactly these clinical trials.
The Protocol: How to Actually Do It
The Dosing Schedule
The Stamets Protocol follows a rhythmic cycle designed to prevent tolerance buildup in the psilocybin component while allowing the neuroplastic changes to stabilize and mature:
4 days ON → 3 days OFF
During the 4 ON days, you take all three components. During the 3 OFF days, you take nothing (though you can continue Lion’s Mane on off days if desired, as it is non-psychoactive and tolerance to it is not a concern).
This weekly cycle is typically repeated for 4 consecutive weeks (one month), followed by a reset period of 2–4 weeks with no psilocybin. Many microdosers repeat multiple rounds over months or choose to cycle indefinitely with regular reset periods.
The Doses
Based on Stamets’ recommendations and the most commonly reported protocol in the microdosing community:
Psilocybin (dried Psilocybe cubensis):
0.1g to 0.3g dried mushrooms — equivalent to approximately 1–3mg of psilocybin. This is the foundational microdose range. Start at 0.1g and adjust based on your sensitivity. If you feel anything perceptual at all, your dose is too high — reduce it.
Lion’s Mane extract:
500mg to 1000mg of a quality Lion’s Mane extract. Stamets recommends mycelium-based extracts as potentially most beneficial for neurological applications, given that erinacines (the most potent neuroactive compounds) are found in the mycelium rather than the fruiting body. That said, fruiting body extracts containing hericenones also have substantial research support.
Niacin (flushing nicotinic acid — not niacinamide):
100mg to 200mg. Start at 50mg if you are sensitive to flushing. Work up gradually. Do not substitute with “no-flush” niacinamide — it does not produce the vasodilation that is central to Stamets’ delivery theory.
Timing
Most practitioners take all three components simultaneously in the morning, on an empty or light stomach, to align the niacin flush with the subtle onset of psilocybin’s effects. Some prefer to take niacin 10–15 minutes before the other two to allow the vasodilation to begin before the psilocybin is absorbed.
What to Expect
On a well-calibrated Stamets Stack, you should feel nothing dramatic. That’s the point. Common reports from long-term stackers include:
A gentle warmth or flush 15–20 minutes after dosing (niacin)
A barely perceptible brightening of mood or mental clarity within 60–90 minutes
Slightly enhanced creative thinking or problem-solving flexibility
A mild feeling of being “more present” or engaged
Reduced emotional reactivity over the course of weeks
Gradual improvements in focus and memory over a 4-week protocol
If you feel visually altered, anxious, dissociated, or noticeably “high” — your psilocybin dose is too high. Reduce it immediately. The goal is sub-perceptual. Always.
Who Is the Stamets Stack For?
Based on community data and the theoretical framework of the Stack, it appears most relevant for:
People interested in cognitive enhancement: The combination of neuroplasticity (psilocybin), NGF stimulation (Lion’s Mane), and improved delivery (niacin) creates a theoretically compelling stack for those seeking to optimize focus, creativity, and memory.
People managing depression or anxiety: Microdosing psilocybin has shown small-to-medium improvements in mood and mental health in observational studies. The Stack adds Lion’s Mane’s independently documented mood-supporting and anti-depressive effects — a meaningful addition for those looking for gentle, consistent support.
Older adults interested in neurological health: The 2022 observational study found that adults over 55 using the full Stack showed greater improvements in psychomotor performance than those using psilocybin alone — one of the most concrete signals to date that the combination may have age-specific benefits.
Anyone interested in long-term brain health: Stamets was motivated primarily by neurodegenerative disease prevention. The combination of psilocybin’s neuroplasticity, Lion’s Mane’s NGF stimulation, and niacin’s circulatory support represents a multi-angle approach to maintaining and enhancing brain function over time.
Who it may NOT be for:
People currently on SSRIs or MAOIs (significant drug interactions possible)
People with a personal or family history of psychosis or schizophrenia
People with a history of liver disease (niacin at high doses can affect liver enzymes)
Pregnant or breastfeeding individuals
Anyone with blood pressure sensitivity (niacin’s vasodilation can interact with blood pressure medications)
Always consult a healthcare professional before beginning any microdosing protocol. And always check our full Microdosing 101 Guide before getting started.
The Stamets Stack vs. The Fadiman Protocol
For those already familiar with microdosing, you may wonder how the Stamets Stack compares to the better-known Fadiman Protocol — named after psychedelic researcher Dr. James Fadiman.
The Fadiman Protocol is simpler: 1 day ON, 2 days OFF, psilocybin only. No supplemental stack.
The key differences:
Frequency: Stamets doses more frequently (4 days on vs. 1 day on). This increases total psilocybin exposure but potentially also tolerance risk — mitigated in the Stack by the 3-day break.
Complexity: Stamets adds Lion’s Mane and niacin; Fadiman uses psilocybin alone. This makes the Stack harder to attribute specific effects to any single component.
Goal orientation: Fadiman’s protocol was developed primarily for general wellbeing and mental health enhancement. The Stamets Stack is specifically oriented toward neurogenesis and long-term neurological optimization.
Evidence: Both protocols have observational data supporting benefits, but neither has robust placebo-controlled clinical trial evidence for the specific regimen as a whole.
Many people make the mistake of starting at the top of the dose range. Psilocybin sensitivity varies enormously. Begin at 0.1g, 50mg niacin, and 500mg Lion’s Mane. Evaluate for one full week before considering any adjustment.
Use Flushing Niacin — Not Niacinamide
This cannot be overstated. Niacinamide is the non-flushing form of B3 — it does not cause vasodilation and does not serve Stamets’ delivery hypothesis. If you’re not flushing, you’re not running the Stack as intended.
Track Your Experience
Keep a simple daily journal. Note mood, focus, creativity, sleep quality, and any unusual sensations. Over a 4-week cycle, patterns emerge that are difficult to perceive day by day but obvious in retrospect.
Choose Quality Lion’s Mane
The Lion’s Mane supplement market is full of products with poor potency, mycelium-on-grain products with minimal erinacine content, or adulterated formulas. Stamets himself recommends mycelium-based extracts for maximum erinacine content. Choose products that clearly specify their extraction method and active compound concentration.
Respect the OFF Days
The 3-day break in the Stamets Protocol serves two purposes: preventing psilocybin tolerance, and allowing the neuroplastic changes stimulated by the ON days to consolidate and mature. Skipping the OFF days undermines both purposes.
Plan Your Integration
Even at microdose levels, the Stamets Stack can surface unexpected emotional material over the course of a full protocol. Journaling, meditation, and regular reflection during the 4-week cycle will help you integrate what arises. Read our Integration Guide for full support.
What Stamets Is Really Claiming — And What He Isn’t
It’s worth being clear about the distinction between what Stamets has theorized, what he has claimed in patents, and what science has confirmed.
What Stamets claims: That the combination of psilocybin, Lion’s Mane, and niacin synergistically promotes neurogenesis, repairs neurological damage, and could benefit conditions ranging from Alzheimer’s and PTSD to general cognitive enhancement in healthy individuals.
What science has confirmed: Each ingredient individually has meaningful neurological activity. Psilocybin promotes neuroplasticity with growing evidence. Lion’s Mane stimulates NGF and BDNF with strong preclinical and growing human evidence. Niacin supports circulation and brain health with independent evidence. The combination has shown a promising signal in a large observational study. The specific synergistic mechanism Stamets proposes has not yet been formally tested in a controlled human trial.
Stamets has been criticized by some in the scientific community for the breadth of his patent claims and the ahead-of-evidence enthusiasm of his public statements. Those criticisms are fair. But the core idea — that combining a neuroplasticity catalyst, a nerve growth factor stimulator, and a circulatory enhancer might produce additive or synergistic neurogenic benefits — is not only plausible but scientifically grounded in the known properties of each compound.
The rigorous trials are coming. The signal is there. And until the controlled data arrives, the Stack remains one of the most scientifically coherent and well-reasoned approaches to neurological optimization available to curious, harm-reduction-oriented individuals.
Frequently Asked Questions
Do I need all three ingredients for the Stack to work?
Stamets designed the Stack with all three working synergistically. However, many people run psilocybin + Lion’s Mane without niacin if the flush is uncomfortable or contraindicated. Some run Lion’s Mane + niacin without psilocybin due to legal restrictions. Each combination has theoretical value, but the full three-ingredient Stack is Stamets’ specific protocol.
Can I take Lion’s Mane on my OFF days?
Yes. Lion’s Mane is non-psychoactive and does not produce tolerance. Many practitioners take it daily regardless of psilocybin dosing days to maintain consistent NGF stimulation.
Will the niacin flush go away over time?
Yes. With regular use, niacin tolerance develops and the flush diminishes — sometimes disappearing almost entirely. Some practitioners take a break from niacin periodically to restore the flush, believing it indicates the vasodilatory mechanism is actively engaged.
Can I use Lion’s Mane capsules instead of fresh mushroom?
Yes. Fresh Lion’s Mane is excellent if available, but quality extract capsules are the most practical format. Stamets recommends mycelium-based extracts for higher erinacine content, though fruiting body extracts with hericenones are also effective. Aim for 500mg–1000mg of a quality extract daily.
Is this the same as the Fadiman Protocol?
No. The Fadiman Protocol uses psilocybin alone on a 1-day-on, 2-days-off schedule. The Stamets Protocol adds Lion’s Mane and niacin on a 4-days-on, 3-days-off schedule. Both are legitimate microdosing protocols with different theoretical bases and practical rhythms.
How do I source the psilocybin component in Canada?
Browse our full selection of psilocybin microdose capsules at Shroom Bros — precisely dosed, consistent quality, and formulated for exactly this kind of protocol.
The Bottom Line
The Stamets Stack is not a magic bullet. It’s not a pharmaceutical. It’s not a proven cure for anything.
What it is: a thoughtfully constructed, theoretically grounded, and increasingly well-observed protocol that combines three compounds with individually meaningful neurological properties — in a configuration designed to address the brain’s neuroplasticity, neurogenesis, and circulatory health simultaneously.
Psilocybin creates the neuroplastic conditions. Lion’s Mane builds through them with nerve growth factors. Niacin drives both compounds deeper into the nervous system where the real work happens. Together, the theory goes, they do something none of them can do alone.
The controlled trials will come. The signal is already there. And for those who approach it with intention, patience, and appropriate medical guidance, the Stamets Stack represents one of the most genuinely interesting experiments in modern cognitive wellness — grounded in the ancient wisdom of fungi and the cutting edge of neuroscience at the same time.
Stamets Patent Application (2018) — “Compositions and methods for enhancing neuroregeneration and cognition by combining mushroom extracts containing active ingredients psilocin or psilocybin with erinacines or hericenones enhanced with niacin” — https://patents.google.com/patent/US20180021326A1/en
Rootman et al. (2021) — “Adults who microdose psychedelics report health-related motivations and lower levels of anxiety and depression compared to non-microdosers” — Scientific Reports — https://pmc.ncbi.nlm.nih.gov/articles/PMC8602275/
Rootman et al. (2022) — “Psilocybin microdosers demonstrate greater observed improvements in mood and mental health at one month relative to non-microdosing controls” — Scientific Reports — https://www.nature.com/articles/s41598-022-14512-3
Shao et al. (2021) — “Psilocybin induces rapid and persistent growth of dendritic spines in frontal cortex in vivo” — Neuron — https://pubmed.ncbi.nlm.nih.gov/34228959/
Disclaimer: This blog is for educational and harm reduction purposes only and is not medical advice. Always consult a healthcare professional before beginning any supplement or microdosing protocol.
Most people who’ve tried magic mushrooms have done so at 1 gram, maybe 2. A comfortable, curious, manageable experience. Colors shift a little. Music sounds better. You feel connected and warm.
Five grams is something else entirely.
“At 5 grams, the world as you know it ceases to exist.”
That’s not an exaggeration. It’s not hype. It’s the honest, reported reality of what happens when a human being consumes what ethnobotanist Terence McKenna famously called a heroic dose — five dried grams of Psilocybe cubensis, taken intentionally and with full commitment.
This post is not a guide on whether you should do it. It’s a detailed, honest, minute-by-minute breakdown of what the heroic dose actually feels like, why it feels that way, and what the science says is happening in your brain while it unfolds.
Read it whether you’re curious, preparing, or simply trying to understand what people mean when they say a mushroom experience changed their life.
Before We Start: What Is the Heroic Dose?
Terence McKenna — the American ethnobotanist, philosopher, and one of the most influential voices in psychedelic culture — coined the term “heroic dose” to describe a very specific method of consumption: five dried grams of Psilocybe cubensis, taken alone, on an empty stomach, in silent darkness, with eyes closed.
McKenna’s framework was intentional. The darkness and silence eliminate external anchors for the mind. The solitude strips away social performance. The empty stomach accelerates onset and maximizes absorption. Together, these conditions create the optimal environment for what McKenna described as a “profound visionary experience.”
DoubleBlind Magazine describes it plainly: unlike high doses, which hover around 3.5 grams or so, heroic doses are strong enough to take you out of your present reality entirely.
The name itself is worth unpacking. “Heroic” doesn’t mean brave in the ordinary sense. It refers to the Hero’s Journey — the archetypal process of personal transformation described in myths and fairy tales across human history. You go in. You are changed. You return different.
Important disclaimer: This blog is for educational and harm reduction purposes. A heroic dose is not a recreational experience. It carries real psychological risks and is not appropriate for everyone. Never attempt a heroic dose without prior lower-dose experience, a safe set and setting, and ideally a trusted sitter or guide present. Read our full Magic Mushroom Safety Guide before proceeding.
What 5 Grams Actually Contains
Before the timeline, a quick pharmacological note: when you eat 5 grams of dried P. cubensis, you’re consuming approximately 30–50 mg of psilocybin — based on average psilocybin content of around 0.5–1% of dry mushroom weight, with a range across species of 0.03% to 1.78%. In Johns Hopkins clinical research, the highest doses studied were 30 mg/70 kg bodyweight — roughly equivalent to 3–5 grams of dried mushrooms. So 5 grams sits at the very top of what clinical researchers consider the high-dose threshold.
At those doses, Johns Hopkins research found that 72% of volunteers had mystical-type experiences, and one month later they rated the session as having substantial personal and spiritual significance, with sustained positive changes in attitudes, mood, and behavior that were still undiminished at 14-month follow-up.
That context matters. The heroic dose isn’t folklore. It’s one of the most rigorously documented psychological experiences in modern science.
For a deeper look at how strain potency affects this equation, check out our complete mushroom strains guide. A Penis Envy 5-gram experience is categorically different from a 5-gram Golden Teacher experience.
The Minute-by-Minute Timeline
What follows is a composite account drawn from community reports, clinical research timelines, and pharmacokinetic data. Every person’s experience differs based on body weight, metabolism, strain potency, stomach contents, emotional state, and environment. But the broad arc — the phases, the transitions, the quality of experience — is remarkably consistent at this dose level.
The clock starts when you swallow.
⏱ Minutes 0–20: Stillness Before the Storm
You’ve eaten. The mushrooms are in your stomach. For the first 15–20 minutes, there’s often nothing detectable happening — just you, your breath, and the quiet awareness that something irreversible has been set in motion.
Most people describe a rising anticipatory tension during this window. Not quite anxiety, not quite excitement — something between the two. Your body knows. Your mind doesn’t yet.
Some people feel mild stomach awareness — a slight gurgling or warmth in the gut as the psilocybin begins its conversion to psilocin in the liver. This is normal, and at this dose, it’s almost a reliable signal that the process has begun. If you’re sensitive to nausea, having consumed your mushrooms in tea or chocolate form will have dramatically reduced this. For a full breakdown of how format affects onset, read our post on mushroom chocolate and bioavailability.
What to do: Lie down. Close your eyes. Set your intention one final time. Breathe slowly. You will not be able to stop what comes next — only receive it.
⏱ Minutes 20–40: First Contact
The first signals arrive. They’re subtle at first — easily mistaken for imagination — and then unmistakably real within minutes of each other.
Visual field shifts. With eyes closed, the darkness behind your eyelids begins to develop texture. Geometric patterns emerge — symmetrical, complex, pulsing faintly at first. Colors that aren’t there begin to accumulate in your peripheral vision. With eyes open, objects begin to breathe. The ceiling undulates. Edges soften.
Body sensations begin. A warmth or electricity moves through your limbs. Some people experience a wave of nausea at this point — especially on dried mushrooms consumed raw — which passes within 10–15 minutes for most. Some people feel a strong urge to yawn or stretch as the body responds to the sudden neurochemical flood.
Time starts to distort. The gap between thoughts stretches. What feels like 20 minutes may have been 5. The ordinary rhythm of your internal clock begins to slip.
At the pharmacological level, psilocin is now binding rapidly to 5-HT2A serotonin receptors concentrated in the prefrontal cortex. Blood levels of psilocin are rising quickly. The brain is beginning to experience what researchers describe as “massively disrupted functional connectivity” — the normal routing of neural signals is breaking down and new, unexpected connections are forming.
The feeling: An elevator beginning to rise. Still inside the building. But moving.
⏱ Minutes 40–60: Liftoff
This is where 5 grams separates itself from every lower dose you’ve ever tried.
The visual field doesn’t just shift — it transforms. With eyes closed, you are no longer in darkness. You’re inside an architectural space of cascading geometric forms: mandalas within mandalas, fractal landscapes that breathe and morph with impossible detail. Colors no longer correspond to anything in the physical world — you’re witnessing hues your waking consciousness has no name for.
Synesthesia begins. Music (if you’re listening to any) becomes visible. Sounds have textures. The boundary between senses starts to dissolve. A high dose brings “kaleidoscope visuals when eyes are closed or open, sensory and perceptual changes, synesthesia like hearing colors or tasting sounds, cognitive changes, and ego dissolution.”
Emotional intensity spikes. Whatever emotional material exists in your psyche — unprocessed grief, old fear, deep love, awe — begins surfacing rapidly and powerfully. This is not random. Psilocin’s action on 5-HT2A receptors disrupts the Default Mode Network (DMN) — the brain’s self-referential processing hub — creating a state in which emotional material bypasses the usual filters of ego-defense and moves directly into awareness. Neuroimaging studies have consistently shown that psychedelics like psilocybin significantly reduce DMN connectivity, and that this correlates directly with the subjective experience of ego dissolution.
Nausea (if present) typically ends here. The transition to peak is often the most physiologically turbulent part of the experience, but as the compound reaches full activity, most GI discomfort passes.
The feeling: You are no longer in the elevator. You’ve cleared the building. You’re above the clouds and still accelerating.
⏱ Hours 1–2: Entering the Deep
Language begins to struggle here. Not because the experience becomes incoherent — but because what is happening falls outside the categories that language was designed to describe.
Reality becomes fluid. The ordinary consensus structure of the world — the agreement that objects are solid, that self and other are separate, that time flows in one direction — loosens its grip entirely. At 5 grams, this is not a partial or metaphorical dissolution. It is literal. You may not know your name. You may not remember that you took mushrooms. You may not have a stable sense of being a person who is having an experience.
Ego dissolution begins. This is the defining feature of the heroic dose and the most difficult to describe to anyone who hasn’t experienced it. The “self” — the internal narrator, the sense of being a distinct person separate from the world — begins to quiet and then disappear. This is not a loss of consciousness. You are fully awake. But the one who is usually awake — “you” — is no longer present in the usual way.
What remains is awareness without a center. Experience without an experiencer. “In a state of ego dissolution, the boundaries are let down and a great zooming out takes place where you begin to see things on a macroscopic level. You are no longer an individual isolated from life as it takes place around you, but rather you are interconnected with everything through the web of life.”
From a neuroscience perspective, ego dissolution happens when the default mode network loses its usual grip and the communication between its hubs weakens. The DMN — which governs self-awareness, internal narrative, and the distinction between self and other — is dramatically suppressed by psilocin. What remains is pure, undifferentiated awareness.
Visions intensify to their maximum depth. At this point, with eyes closed, the visual content moves beyond geometry into full visionary experience. Landscapes. Faces. Beings. Symbolic narratives. Many people at this dose level describe encountering presences or entities — not experienced as hallucinations, but as encounters with something genuinely outside themselves. Whether this is neurological, philosophical, or spiritual is a question that science has not answered. What is documented is that it is experienced as profoundly real.
Time becomes irrelevant. The heroic dose produces its effects for 6 to 8 hours — but as time dilates during a trip of this kind, one’s perception of the time frame becomes far beyond that of ordinary measured time. What feels like lifetimes may be minutes. Many people report that subjective time during peak ego dissolution feels essentially infinite — not long, but dimensionless.
The feeling: You are not in a place. You are not a person. There is only this.
⏱ Hours 2–4: The Peak — Where the Work Happens
A heroic dose has three phases: the blast off, which usually happens within the first two hours; the strongest or peak experience, which occurs from around hours 2 to 4; and the comedown.
For many people, this is the most significant period of their lives. Not most significant drug experience. Most significant experience.
What commonly occurs at peak:
Complete mystical experience — a sense of profound unity with all things, transcendence of time and space, overwhelming positive mood, and an encounter with something felt as sacred or ultimate. Johns Hopkins research using the Mystical Experience Questionnaire found that at high doses, 72% of participants reported mystical-type experiences, and these were rated among the five most meaningful and spiritually significant events of their lives — more meaningful than the birth of a child or the death of a parent.
Emotional catharsis — grief, love, fear, joy, and awe flowing without the usual dams of ego-defense. People cry. People laugh. People face things they’ve been running from for years. The psychedelic process does not let you choose what surfaces.
Challenging experiences — it’s critical to acknowledge that at this dose, difficult experiences are common and expected. Johns Hopkins data shows that at high doses, 39% of volunteers experienced extreme anxiety or fear at some point during the session. This is not a failure of the experience — it is often the most therapeutically significant part of it. The ability to move through difficulty, to practice surrender rather than resistance, is exactly what the heroic dose asks of you.
Profound insight — about your life, your relationships, your patterns, your deepest fears and desires. These insights often feel more real and certain than anything you’ve understood before. Many persist long after the compound has cleared.
The neuroscience of the peak: Your brain is in a state that has no everyday analogue. Psilocybin has massively disrupted functional connectivity across cortex and subcortex — with research published in Nature showing this disruption is more than threefold greater than that of stimulant drugs. The brain’s usual specialized networks have dissolved into a state of massive global communication — sometimes called the “entropic brain” — in which every region is talking to every other region simultaneously. This is what produces the sense of universal connection, the dissolution of boundaries, and the perception that everything is deeply, meaningfully interrelated.
The feeling: Impossible to describe. People use words like birth, death, God, everything, nothing, home, ancient, infinite. Whatever it is, it is felt — with total certainty — as more real than ordinary reality.
⏱ Hours 4–5: The Tide Begins to Turn
Slowly — and it is slow — the peak begins to soften.
The return of self happens in fragments. A thought arrives that sounds distinctly like you. Then another. The geometric architecture of the closed-eye visual field begins to simplify. The undulations in the physical environment slow and soften. You begin to remember that you took mushrooms. You begin to remember your name.
This is often one of the most emotionally resonant phases of the entire experience — the return. There is frequently a profound sense of gratitude, of having been somewhere enormous and been returned to the ordinary world with something new. Many people cry during re-entry. Not from sadness — from the sheer intensity of the contrast between where they’ve been and the ordinary miracle of simply being alive.
Physical sensations return to the foreground. You may feel genuinely exhausted — the body has been running at neurological full capacity for hours. Mild jaw tension, a sense of physical weight, and deep fatigue are common. Drink water. Stay warm. Don’t rush to move.
The feeling: A ship returning to harbor after an enormous voyage. The sea is still moving. You can feel the difference in your body.
⏱ Hours 5–8: Resolution and Afterglow
The fully psychedelic phase is over. But the experience is not.
What remains is what the psychedelic community calls the afterglow — a period of unusual clarity, emotional softness, and perceptual richness that can last anywhere from a few hours to the following day. Music sounds beautiful. Food tastes vivid. Conversations feel meaningful in ways that ordinary conversation doesn’t.
Cognitive processing is active. Your mind is quietly beginning to organize and integrate what just happened. Insights surface in gentle, conversational form rather than overwhelming waves. This is an excellent time to begin journaling — even rough, half-formed notes — because the vividness of the experience fades faster than most people expect.
Emotional sensitivity remains elevated. Some people feel euphoric. Some feel fragile and tender. Some feel profoundly peaceful. All of these are valid and expected. Avoid stimulating environments, bright screens, or demanding social interactions during this window. Your nervous system has been through something significant and deserves care.
The feeling: Standing outside after a thunderstorm. Everything is quiet. The air is different. So are you.
What Happens in Your Brain: The Neuroscience Summary
For those who want to understand the biology underneath the experience:
The Default Mode Network Goes Offline
The DMN is the brain network responsible for self-referential thought — your internal narrative, your sense of being a distinct self, your rumination, your autobiographical memory. Psychedelics dramatically reduce DMN connectivity, and this reduction correlates directly with ego dissolution. When the DMN loses its grip, the sense of a bounded, separate self disappears — which is experienced as unity, oneness, or the dissolution of the ego.
Researchers at Imperial College London found that this “resetting” of the DMN is likely linked to psilocybin’s antidepressant effects — turning off the rigid self-referential loops associated with depression and reconsolidating them in a more flexible, less rigid form.
Global Brain Connectivity Explodes
Normally, different brain networks operate in isolation — the visual network, the auditory network, the emotional network, and so on. Psilocybin breaks down this segregation, creating vast cross-linking between networks that don’t normally communicate. This increased global connectivity is what produces synesthesia (hearing colors, seeing sounds), the sense that everything is connected, and the perception of visionary content with no external stimulus.
New Neural Connections Begin Forming
As we covered in our blog on Psilocybin and Neuroplasticity, a landmark 2021 Yale study showed that a single psilocybin dose produces approximately a 10% increase in dendritic spine density in the prefrontal cortex — new physical connections between neurons — within 24 hours, that persist for at least a month. The neural activity during your experience shapes which connections are built. What you think, feel, and process during the trip becomes, quite literally, new brain architecture.
This is why integration matters so much after a heroic dose. You’re not just processing an experience emotionally — you’re tending to new neural construction.
The Aftermath: What Changes
People don’t take heroic doses for entertainment. They take them because something needs to shift — and the evidence suggests it does.
Johns Hopkins research has documented that a single high-dose psilocybin session, combined with preparation and integration, produces:
Significant reductions in depression and anxiety persisting for 6–12 months
Increased psychological openness and flexibility
Lasting changes in attitudes toward life, self, and others
Reduced fear of death in patients with life-threatening illness
More than 85% of participants rating the experience as one of the five most meaningful and spiritually significant of their lives
These are not small effects. These are among the largest and most sustained psychological outcomes ever measured in a clinical trial.
The heroic dose is not magic. It is not a guaranteed cure for anything. But at its best — properly prepared, properly supported, properly integrated — it is one of the most powerful tools available to the human mind for breaking patterns, dissolving defenses, and encountering the deeper layers of who you are.
Before You Consider It: The Essential Checklist
✅ Prerequisites
Extensive experience at lower doses (1g → 2g → 3.5g minimum, over multiple sessions)
No personal or family history of psychosis, schizophrenia, or bipolar disorder
Not currently on SSRIs, MAOIs, or lithium
A trusted sitter present or immediately reachable
A safe, private, comfortable physical environment
Clear intention set in advance
An empty or near-empty stomach (3–4 hours fasted minimum)
An integration plan for the days and weeks following
✅ Strain Matters
Do not attempt a heroic dose with a high-potency strain like Penis Envy unless you are deeply experienced. Experienced users recommend starting a 5-gram heroic dose with a moderate-potency strain like Golden Teacher or a similar cultivar. Check our full strain effects guide before selecting.
✅ Integration Is Non-Negotiable
The weeks following a heroic dose are a critical neurological window — new dendritic spines are maturing, new neural pathways are consolidating. Journal. Sleep. Move your body. Speak with a therapist or integration coach if possible. Don’t rush back to ordinary routine. For everything you need to know, read our Psilocybin Integration Guide.
Frequently Asked Questions
Is 5 grams the same for everyone?
No. Mushroom potency varies enormously by strain and batch. A 5-gram heroic dose of Golden Teacher is a very different experience from 5 grams of Penis Envy — which could be 2–3x more potent. Always know your strain, and always work up gradually. A dose that is “heroic” for one person may be moderate for another.
Will I lose control of my body?
At a true heroic dose, most people are lying still with eyes closed. Gross motor function remains intact — you can move, stand, and seek help if needed. However, your capacity for coordinated, purposeful action is significantly impaired for several hours. This is one of the most important reasons for having a sitter present.
What if it goes badly?
Difficult experiences at this dose are common and often the most therapeutically meaningful. The primary harm-reduction tool is surrender — resisting a difficult experience amplifies it, while accepting and moving toward it tends to move it through. Having a trusted, sober sitter who understands psychedelics and can provide calm, grounding presence is the single most important safety factor at this dose level.
How long until I should do it again?
McKenna himself advocated for infrequent use. He recommended no more than two to three times per year at this dose level. The neuroplasticity research supports this — new connections need weeks to mature and stabilize before the process is repeated. The standard community recommendation is a minimum of 30 days between high-dose sessions, and many experienced users wait much longer.
Is this the same as what happens in clinical trials?
Clinical trial doses typically range from 20–30 mg of pharmaceutical-grade psilocybin, which roughly corresponds to 2.5–5 grams of dried cubensis. The experiences described in clinical research — mystical states, ego dissolution, profound emotional processing — are qualitatively consistent with what community users report at the heroic dose. The key difference is the presence of professional therapists, a clinically optimized environment, and formal integration support. The experience itself is the same.
The Bottom Line
Five grams of dried magic mushrooms is not a party. It’s not a night out. It’s not a way to get high.
It is — if approached correctly — one of the most profound experiences available to the human mind. A full dissolution of the ordinary sense of self. A direct encounter with something that most people describe as larger than any category their usual consciousness contains. And, consistently, an experience that is rated months and years later as among the most meaningful of an entire lifetime.
The timeline above is a map. But maps are not the territory. No description — not this one, not any — can prepare you for what 5 grams actually feels like. The preparation, the intention, the surrender, the integration: those are the real work. The compound just opens the door.
Griffiths et al. (2016) — “Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer” — Journal of Psychopharmacology — https://pmc.ncbi.nlm.nih.gov/articles/PMC5367557/
Disclaimer: This blog is for educational and harm reduction purposes only and is not medical advice. Psilocybin mushrooms are a controlled substance in many jurisdictions. Always research the laws in your area before proceeding.
There’s a question that comes up constantly in the mushroom community: “I took 1 gram and it hit way harder than when I ate dried mushrooms at the same dose. What gives?”
It’s not your imagination. It’s not a batch that was somehow stronger. It’s not a placebo.
When you consume psilocybin in chocolate form — or in a gummy, or in a capsule — your body processes it differently than it does when you chew through a handful of dried Psilocybe cubensis. The matrix the compound is delivered in changes everything: the onset, the peak, the smoothness, the intensity, and even the duration.
This blog breaks down exactly why 1 gram in a chocolate bar is not the same as 1 gram of raw dried mushrooms — and what that means for how you should approach dosing.
First, Let’s Talk About What Psilocybin Actually Is
Before we get into the chocolate science, a quick primer.
Psilocybin is the compound in magic mushrooms that makes them magic. But here’s the thing — psilocybin itself is technically inactive. It’s what pharmacologists call a prodrug. When you ingest it, your body converts it into psilocin, the compound that actually binds to your serotonin receptors and produces the psychedelic experience.
This conversion happens primarily in the liver through a process called dephosphorylation. The speed and completeness of that conversion — and how efficiently psilocin enters your bloodstream — is where the differences between consumption methods start to emerge.
Pharmacokinetic research shows that after oral administration, psilocybin is detectable in the bloodstream within 20 to 40 minutes, with psilocin peak levels typically arriving between 1 and 3 hours depending on the individual and method of consumption. But that window shifts significantly depending on what vehicle is carrying the psilocybin into your body.
If you want a broader overview of how psilocybin affects you once it’s in your system, our guide on How Shrooms Make You Feel is a great foundation.
The Real Reason Dried Mushrooms Are Harder to Digest Than You Think
Here’s something most people don’t think about: when you eat dried mushrooms, you’re not just eating psilocybin. You’re eating an entire organism — cell walls, fibres, proteins, polysaccharides, and all.
The cell walls of fungi are made of chitin (pronounced “KYE-tin”) — the same tough structural compound found in crab shells and insect exoskeletons. Chitin is notoriously difficult for the human body to break down. Your digestive system doesn’t produce the enzymes needed to fully dissolve it, which means two things happen when you eat raw dried mushrooms:
Absorption is delayed and inconsistent. Psilocybin locked inside intact chitin cell walls takes longer to escape into your digestive system, leading to a slower, more unpredictable onset.
Nausea is common. Chitin irritates the gastrointestinal tract. It triggers inflammatory and immune responses in the gut, which contributes to the infamous “gut rot” that many mushroom users experience in the first 30–60 minutes of a trip.
As mycologist Paul Stamets has noted, “raw mushrooms are largely indigestible because of their tough cell walls, mainly composed of chitin.” Raw mushrooms may even contain heat-sensitive compounds and pathogens that the body tries to expel — which is part of why nausea can be intense with unprocessed dried material.
This is the foundational reason why edible forms of psilocybin — chocolates, gummies, capsules, and teas — can feel so different. They bypass or reduce the chitin problem entirely.
What Happens When Mushrooms Are Processed Into Chocolate
When mushrooms are prepared for a chocolate bar, the process typically involves grinding the dried mushrooms into a fine powder and incorporating that powder into a chocolate matrix. This matters for several reasons.
1. Cell Wall Disruption Increases Bioavailability
Grinding dried mushrooms into a powder mechanically ruptures the chitin cell walls that normally slow absorption. More surface area is exposed, which means psilocybin leaches out into your digestive system more quickly and more completely than it would from a whole or coarsely chewed mushroom.
2. Fat Content in Chocolate Affects Absorption Timing
Chocolate contains significant amounts of fat — primarily cocoa butter. Fats slow gastric emptying, which means the contents of your stomach move more gradually into your small intestine (where most absorption occurs). This produces a classic edible effect: a delayed onset followed by a more sustained, even release of the active compound.
The fats and sugars in the chocolate matrix can slow gastric emptying, potentially delaying initial effects while extending overall duration. This is why many people describe mushroom chocolate experiences as having a softer, more gradual come-up compared to eating raw dried mushrooms — which tend to hit harder and faster on an empty stomach.
3. Gummies Are Different Again
Gummies add another layer of distinction. Many high-quality mushroom gummies are made with psilocybin extract rather than ground whole mushroom matter. This means there’s no chitin to deal with at all — just the active compound in a gelatin or pectin delivery matrix.
Gummies often contain just psilocybin extract and no mushroom matter, which is why you generally shouldn’t experience the nausea or muscle cramps that can come with raw mushroom consumption. The tradeoff is that without the full spectrum of compounds found in whole mushrooms, you may lose some of the entourage effects that whole-fruiting-body consumption provides.
The Stomach Environment and Why It Changes Everything
One factor almost nobody talks about when comparing edible formats is the role of stomach acidity and fullness at the time of consumption.
Psilocybin conversion to psilocin happens largely in the liver — but the speed at which psilocybin reaches the liver depends heavily on how quickly it moves through your stomach. An empty, acidic stomach is a very different environment than one that’s full and buffered by fats and carbohydrates.
Empty stomach + dried mushrooms: Fast gastric emptying, chitin irritation, potentially intense and fast onset with significant nausea risk.
Full stomach + mushroom chocolate: Slowed gastric emptying due to fat and sugar content, longer onset (sometimes 90 minutes to 2 hours), smoother peak, reduced nausea.
Empty stomach + mushroom chocolate: Faster than full-stomach chocolate, still smoother than raw dried mushrooms due to powder format and lack of raw fungal matter.
This is critical for dosing. If you ate 1 gram of dried mushrooms on an empty stomach last time and now you’re eating 1 gram of mushroom chocolate after a meal — you are having a fundamentally different pharmacokinetic experience, even at the same gram weight.
The Cacao Chemistry: Why Chocolate Isn’t Just a Delivery Vehicle
Here’s where things get genuinely fascinating. Chocolate isn’t just a neutral wrapper for psilocybin. The cacao itself is pharmacologically active — and it may directly potentiate the effects of psilocybin.
Cacao as a Mild MAOI
Cacao contains naturally occurring compounds called monoamine oxidase inhibitors (MAOIs). Specifically, research has identified tetrahydro-beta-carbolines in cacao — compounds that slow the breakdown of tryptamine alkaloids, including psilocin, in the body.
MAO (monoamine oxidase) is an enzyme responsible for breaking down serotonin and other neurotransmitters — including psilocin — in your gut and bloodstream. When MAO activity is reduced, more psilocin survives and remains active for longer. This is the same basic mechanism behind ayahuasca, where the MAOI-containing plant prevents DMT from being broken down before it can produce effects.
Cacao is not a strong MAOI by any means. But in sufficient quantities, it is thought to produce a mild MAOI effect that can potentiate and extend the effects of psilocybin. The Aztecs were almost certainly aware of this synergy — even if they didn’t have the biochemical language to describe it.
Theobromine: The Heart-Opener
Cacao beans contain up to 40–50% fat and are rich in theobromine — one of the main compounds responsible for their uplifting and stimulating properties. Theobromine is a mild stimulant that can complement the energizing aspects of a psilocybin experience, while also acting as a vasodilator — meaning it widens blood vessels and increases blood flow throughout the body, including to the brain.
Anandamide and PEA
Cacao also contains anandamide — sometimes called the “bliss molecule” — a naturally occurring cannabinoid that produces feelings of euphoria by reducing pain, stress, and anxiety. Cacao also contains enzyme inhibitors that slow the breakdown of anandamide in the body, prolonging its effects.
Additionally, cacao contains phenylethylamine (PEA), sometimes called the “love molecule,” which produces stimulant and mood-elevating effects. The combination of theobromine, anandamide, PEA, and mild MAOI activity means that the chocolate in your mushroom bar is not passive — it’s contributing its own pharmacological fingerprint to the experience.
This ancient biochemical synergy is almost certainly why the Aztecs combined these two “foods of the gods” for thousands of years in their ceremonial practice.
The Ancient Aztec Combo: They Knew Before We Did
The combination of cacao and psilocybin mushrooms is not a modern invention. Thousands of years ago, the Aztecs and other Mesoamerican cultures were knowingly combining cacao with the transformative power of psilocybin mushrooms in sacred ceremony. This ancient combination was referred to as “cacahua-xochitl” — literally meaning “chocolate-mushrooms.”
The Aztecs combined psilocybin mushrooms with admixtures containing honey, flowers, and herbs, according to records of Aztec history. During the ceremony, the Aztecs would reportedly drink the cacao first, then eat the psilocybin mushrooms with honey.
We now know that cacao contains small amounts of enzyme inhibitors capable of slowing the breakdown of the psychoactive compounds found in psilocybin mushrooms, thereby perpetuating or amplifying the effects. The Aztecs may not have had the biochemical language — but they had thousands of years of empirical observation.
Dosing Mushroom Chocolates: What 1 Gram Actually Means
So with all of this context — what does 1 gram in a chocolate bar actually mean?
The Potency Variable: What Kind of Mushroom Was Used?
Not all mushroom chocolates are created equal. The psilocybin content of magic mushrooms varies enormously — even within the same species. Psilocybin content typically ranges from around 0.5% to 1% of the dried weight of the mushroom, with a range of 0.03% to 1.78%. A 1 gram bar made with Penis Envy — one of the most potent strains available — will hit dramatically harder than a 1 gram bar made with a lower-potency Golden Teacher or B+ strain.
This is a crucial distinction that many consumers overlook. When a bar says “1g,” that’s the weight of mushroom material — not the weight of psilocybin. The actual psilocybin content depends entirely on which strain was used and how it was cultivated.
Check out our breakdown of magic mushroom strains to understand the potency differences between popular varieties.
Distribution: The Hot Spot Problem
Here’s a dirty secret about homemade and low-quality mushroom chocolates: psilocybin doesn’t distribute evenly through chocolate without proper technique.
When mushroom powder is added to melted chocolate without careful, thorough mixing, the powder can clump and settle in certain areas of the bar. This creates what are sometimes called “hot spots” — sections of the bar with significantly more psilocybin than others. You might eat what you think is one square (a quarter gram) and actually consume the equivalent of two grams — or almost nothing.
Professional manufacturers strive to ensure an even distribution of psilocybin throughout chocolate bars, but amateur producers may create hot spots with concentrated doses in specific pieces. This inconsistency is one of the primary reasons why dosing mushroom chocolates can feel so unpredictable — especially with bars from unverified sources.
The Fat-Delay Factor: Why Timing and Fullness Matter
As we covered above, the fat content in chocolate slows gastric emptying. This means:
Don’t redose too early. Many people make the mistake of eating a square, waiting 45 minutes, feeling nothing significant, and eating another square — only to have both doses hit simultaneously when gastric emptying finally occurs. This is how people accidentally overwhelm themselves on what they thought was a moderate dose.
Wait at least 90 minutes before considering a redose. Chocolate edibles can take up to two hours to fully onset depending on your metabolism and what else is in your stomach.
Your last meal matters. A heavy, fatty meal before your chocolate can delay onset even further. A light meal or empty stomach will bring it on faster and more intensely.
The Cacao Potentiation Factor
If you’re comparing your mushroom chocolate experience to a previous dried mushroom experience at the “same” dose — remember to factor in the cacao chemistry. The mild MAOI activity, theobromine, anandamide, and PEA in the chocolate matrix may be contributing to a noticeably stronger or more euphoric experience even before you account for any absorption or distribution differences.
This is especially relevant with ceremonial-grade or high-cacao-percentage chocolate bases. A 70% dark chocolate bar is going to have more active cacao compounds than a milk chocolate base — and may produce a meaningfully different experience at the same mushroom dose.
Practical Dosing Guidelines for Mushroom Chocolates
For Beginners: Start Lower Than You Think You Need To
If you’re new to mushroom chocolates or edibles in general, start with 0.5g–1g and wait a full 90 minutes before evaluating. The delayed onset of fat-based edibles means you need to be patient. A common beginner mistake is to dose at 1g, feel very little at 45 minutes, eat another gram, and then get hit by 2g all at once.
Recreational doses of psilocybin mushrooms are typically between 1.0 and 3.5–5.0 g of dry mushrooms — but in chocolate form, with the factors we’ve discussed, many people find the lower end of that range produces a fuller experience than expected.
For Experienced Users: Scale Cautiously
Even experienced mushroom users should reduce their expected dose by 10–20% when switching from dried mushrooms to chocolate. The smoother, more even absorption — combined with cacao’s mild potentiation — means the same gram weight often produces a more intense experience in chocolate form.
Source Matters Enormously
Given the real risks of uneven distribution in amateur bars, and the documented presence of undisclosed or mislabelled ingredients in unregulated edibles, sourcing your mushroom chocolates from a trustworthy vendor is not optional — it’s essential.
Browse our full selection of mushroom chocolates and mushroom gummies from Shroom Bros — lab-quality sourcing, reliable potency, and consistent distribution every time.
Consider Microdosing Formats for Precision
If consistent, precise dosing is your primary goal — especially for therapeutic or productivity-focused use — microdose capsules offer the most reliable and measurable format. Capsules eliminate the fat-delay variable, the distribution inconsistency, and the cacao potentiation factor, giving you a cleaner baseline from which to calibrate your experience.
For everything you need to know about getting started, read our full Microdosing 101 Guide.
Frequently Asked Questions
Why did my mushroom chocolate hit harder than the same dose of dried shrooms?
Several reasons work together: the mushroom powder in chocolate is more bioavailable than whole dried mushrooms because cell walls are already disrupted; the fat matrix delivers a slower, more complete release; and cacao’s mild MAOI activity, theobromine, and anandamide may genuinely amplify the experience. All of these factors compound on top of each other.
Can I just eat more chocolate to increase the dose?
Yes, but proceed slowly. Because of the delayed onset with fat-based edibles, always wait at least 90 minutes before considering an additional dose. Rushing the redose is the number one cause of accidental overconsumption with mushroom chocolates.
Do mushroom gummies feel different from mushroom chocolates?
Yes, meaningfully so. Gummies — especially those made with psilocybin extract rather than whole mushroom powder — tend to have a faster and more consistent onset, lower nausea risk, and a cleaner come-up without the additional pharmacological contributions of cacao. The trade-off is that they may lack the entourage effect of whole-mushroom products.
Does the percentage of cacao in the chocolate matter?
It can. Higher-cacao-percentage chocolates (70%+ dark chocolate) contain more theobromine, MAOIs, and anandamide than milk chocolate formulations. If you’re eating a ceremonial-grade dark chocolate bar, you may want to start with a slightly lower mushroom dose than you would with a milk chocolate base.
Is heating the mushrooms in the chocolate making the psilocybin weaker?
This is a common concern. The melting point of cacao paste is around 94°F — well below temperatures that degrade psilocybin. Authors of the Psilocybin Chef Cookbook note there’s no hard evidence that typical chocolate-making temperatures meaningfully affect psilocybin content. The benefits of processing (cell wall disruption, reduced nausea) far outweigh any minimal thermal degradation risk in a properly made bar.
The Bottom Line
When you eat 1 gram of psilocybin mushroom chocolate, you are not having the same experience as eating 1 gram of dried mushrooms. You’re consuming a fundamentally different delivery format — one where the mushroom powder has had its cell walls disrupted for better bioavailability, where the fat matrix smooths and extends absorption, and where cacao itself is adding its own mild pharmacological layer to the experience.
The result is typically a softer onset, a longer and more sustained peak, dramatically less nausea — and often a noticeably more intense experience at the same gram weight.
Understanding this isn’t just interesting — it’s essential for dosing intelligently and staying safe. Start lower than you think you need to. Wait longer than you think you should. And respect the fact that the matrix matters as much as the molecule.
There’s a question that comes up a lot in the mushroom community: “Why does a single trip sometimes change the way I feel for weeks or even months afterward?”
It’s a fair question. Psilocybin is out of your system within hours. The trip is over by bedtime. So why do the benefits — the lifted mood, the new perspective, the feeling that something fundamental has shifted — stick around so long after the compound is gone?
The answer, according to a growing body of neuroscience research, is that psilocybin doesn’t just change the way you think. It changes the physical structure of your brain.
We’re talking about real, measurable, microscopic growth — new connections between neurons that weren’t there before. And the most exciting part? These changes happen fast, and they last.
This blog breaks down the science in plain language. No PhD required. Just curiosity.
First, a Quick Brain Anatomy Lesson (We’ll Keep It Simple)
To understand what psilocybin does to your brain, you need to know about three things: neurons, dendrites, and dendritic spines.
Neurons are your brain cells. You have roughly 86 billion of them. They communicate with each other by sending electrical and chemical signals across tiny gaps called synapses.
Dendrites are the branch-like extensions that stick out from each neuron. Think of them like antennae — they receive incoming signals from other neurons.
Dendritic spines are tiny mushroom-shaped bumps that sit along those dendrites. Each spine is a connection point — a place where one neuron receives a signal from another. The more spines you have, and the bigger they are, the more connections your brain can make. More connections means better communication between brain regions, faster processing, and greater cognitive and emotional flexibility.
Here’s the critical part: depression, chronic stress, and anxiety physically shrink and destroy these dendritic spines. People with major depression have measurably fewer spines — especially in the prefrontal cortex, the region responsible for mood regulation, decision-making, and self-awareness. If you want to understand more about how psilocybin interacts with this part of the brain, our blog on How Shrooms Make You Feel is a great starting point.
Depression literally strips your brain of connections. And that’s where psilocybin comes in.
The Yale Study That Changed Everything (2021)
In July 2021, a research team at Yale University published a study in the journal Neuron that sent shockwaves through the neuroscience world. Led by Dr. Alex Kwan, an associate professor of psychiatry and neuroscience, the study provided the first direct evidence that a single dose of psilocybin physically grows new neural connections in a living mammalian brain.
Here’s what they did: using an advanced technique called chronic two-photon microscopy, Kwan’s team tracked 1,820 individual dendritic spines in the frontal cortex of living mice over multiple days. They gave one group a single dose of psilocybin and the other a saline placebo, then watched what happened.
The results were striking.
Within 24 hours of a single psilocybin dose, the mice showed approximately a 10% increase in both the number and size of dendritic spines in the medial frontal cortex — the mouse equivalent of the human prefrontal cortex.
But here’s the part that really made headlines: those new connections were still there a month later.
Dr. Kwan put it plainly: “We not only saw a 10% increase in the number of neuronal connections, but also they were on average about 10% larger, so the connections were stronger as well. It was a real surprise to see such enduring changes from just one dose of psilocybin.”
The study also found that psilocybin reversed stress-related behavioral deficits in the mice and boosted excitatory neurotransmission — meaning not only were the new connections growing, they were actively communicating.
This was huge. For the first time, researchers could literally see psilocybin building new brain architecture, one spine at a time.
Why This Matters for Depression
Remember those dendritic spines we talked about? Depression destroys them. The prefrontal cortex of a person with chronic depression looks physically different under a microscope — fewer spines, thinner dendrites, weaker connections.
Traditional antidepressants like SSRIs work by increasing the availability of serotonin in the brain. But they don’t directly rebuild lost connections. They manage symptoms, often for years, without addressing the underlying structural damage. And they can take 4–6 weeks to produce noticeable effects.
Psilocybin appears to work differently. Instead of just adjusting brain chemistry, it promotes the physical regrowth of the neural infrastructure that depression erodes. And it does it fast — within 24 hours.
This is why a single psilocybin experience can produce antidepressant effects that last weeks or months. It’s not just a chemical mood boost that wears off. The brain has physically rebuilt connections that support healthier patterns of thought and emotion. The hardware has been upgraded, not just the software.
Multiple clinical trials — from Johns Hopkins, Imperial College London, and NYU — have shown that one or two doses of psilocybin, combined with psychotherapy, can produce significant reductions in depression and anxiety that persist for 6 to 12 months. The Yale spine density research gives us a plausible biological explanation for why.
The 2025 Follow-Up: Psilocybin Rewires Entire Brain Networks
The Yale team didn’t stop there. In December 2025, Kwan’s lab (now at Cornell University) published a follow-up study in the journal Cell that went even deeper.
The original 2021 study showed that psilocybin grows new spines. But it left a key question unanswered: where do those new connections lead? Growing spines is great, but if they’re connecting to random neurons, that’s not necessarily therapeutic. The team needed to map which brain regions were being wired together.
To do this, they used an ingeniously modified rabies virus — engineered to jump from neuron to neuron without causing disease — as a biological GPS system to trace psilocybin’s rewiring across the entire mouse brain.
What they found was remarkable: psilocybin’s rewiring is network-specific. It doesn’t randomly grow connections everywhere. Instead, it selectively strengthens pathways from sensory and medial brain regions (the mouse equivalent of the human default mode network) to subcortical targets involved in action and emotion. At the same time, it weakens cortico-cortical feedback loops — the recurrent neural circuits associated with rumination and repetitive negative thinking.
In plain language: psilocybin breaks the mental loops that keep you stuck in depressive thought patterns while simultaneously building stronger connections between perception, emotion, and action.
As Kwan explained: “Rumination is one of the main points for depression, where people have this unhealthy focus and they keep dwelling on the same negative thoughts. By reducing some of these feedback loops, our findings are consistent with the interpretation that psilocybin may rewire the brain to break, or at least weaken, that cycle.”
This study also confirmed something important: the rewiring is activity-dependent. That means the new connections aren’t random — they’re shaped by the neural activity that occurs during the psilocybin experience itself. The trip matters. The thoughts, emotions, and insights you have during your journey are literally sculpting your brain’s new architecture in real time.
How Psilocybin Triggers Neuroplasticity: The Molecular Pathway
So how does a single molecule trigger all of this structural change? Let’s trace the pathway.
Step 1: Psilocin Activates Serotonin 2A Receptors
When you consume magic mushrooms, your body converts psilocybin into psilocin. Psilocin binds to serotonin 2A receptors (5-HT2A), which are densely concentrated on the apical dendrites of pyramidal neurons in the prefrontal cortex — the exact cells where spine growth occurs. A 2025 study published in Nature by Kwan’s team confirmed that psilocybin’s lasting structural effects specifically require 5-HT2A receptors and particular pyramidal cell types.
Step 2: BDNF and mTOR Pathways Are Activated
When those receptors are stimulated, they trigger a cascade of intracellular signaling pathways. The two most important are:
BDNF (Brain-Derived Neurotrophic Factor): Often called “fertilizer for the brain,” BDNF is a protein that promotes the survival, growth, and differentiation of neurons. Psilocybin has been shown to increase BDNF expression. A 2023 study published in Nature Neuroscience found that psychedelics promote plasticity by directly binding to the BDNF receptor TrkB — suggesting a mechanism independent of, or complementary to, 5-HT2A activation.
mTOR (mammalian Target of Rapamycin): This signaling pathway regulates cell growth and protein synthesis. When activated, it promotes the formation of new dendritic spines and synaptic connections. Psilocybin activates mTOR in the prefrontal cortex, directly driving spine growth.
Step 3: New Spines Form and Mature
Within hours of psilocybin administration, new dendritic spines begin to appear. These nascent spines take about 4 days to mature into functional synapses. The Yale study showed that a fraction of these psilocybin-induced spines remained stable for at least a month, suggesting they’ve been fully integrated into the brain’s circuitry.
Step 4: Excitatory Neurotransmission Increases
The new spines aren’t just structural — they’re functional. The Yale team measured increases in miniature excitatory postsynaptic currents (mEPSCs), confirming that the newly grown connections are actively transmitting signals. The brain isn’t just growing new hardware; it’s turning it on.
What About Microdosing?
Most of the spine density research has been conducted with full psychedelic doses. But what about microdosing?
The honest answer: we don’t know for certain yet. There are far fewer studies on microdose-level neuroplasticity. But there’s reason to be optimistic.
A 2024 study published in the Journal of Psychopharmacology found that psilocybin promotes neuroplasticity and produces antidepressant-like effects in mice at varying doses. Preclinical evidence from the OPEN Foundation’s systematic review shows that neuroplastic effects — including elevated BDNF, spine density changes, and neurogenesis markers — appear in a dose-dependent manner, with even lower doses producing measurable effects in some studies.
There’s also the indirect evidence from the Stamets Protocol (psilocybin stacked with Lion’s Mane and Niacin), which Paul Stamets theorizes could amplify neuroplastic effects at sub-perceptual doses. Lion’s Mane independently stimulates Nerve Growth Factor (NGF), potentially complementing psilocybin’s effects on BDNF and spine growth. If you’re curious about microdose capsules that use these kinds of blends, check out our Microdose Capsules: Benefits, Blends, and What to Expect.
The bottom line: full doses have the strongest evidence for structural neuroplasticity. But microdosing likely contributes to neuroplastic change too — we just need more studies to confirm the dose-response relationship.
Psilocybin vs. Traditional Antidepressants: A Different Approach to the Same Problem
Traditional SSRIs (like Zoloft, Prozac, and Lexapro) increase serotonin availability in the brain. They can be effective for many people, but they come with significant limitations:
They take 4–6 weeks to produce noticeable effects
They must be taken daily, often for years or indefinitely
They come with side effects like weight gain, sexual dysfunction, and emotional blunting
They don’t appear to directly rebuild lost neural connections
Stopping them can cause withdrawal symptoms
Psilocybin works through a fundamentally different mechanism. Rather than chronically modulating serotonin levels, it produces an acute burst of 5-HT2A activation that triggers a cascade of structural changes — new spines, new connections, new pathways — that persist long after the compound has left the body.
It’s the difference between taking a daily supplement to manage a deficiency versus doing a single intensive treatment that repairs the underlying damage.
That said, psilocybin isn’t a replacement for SSRIs for everyone. It’s not FDA-approved for depression (yet). It requires careful preparation, the right setting, and ideally professional guidance. And it’s not appropriate for people with certain conditions like schizophrenia or a family history of psychosis. But the neuroplasticity research makes a compelling case that psilocybin addresses depression at a deeper, structural level than most current treatments.
The Bigger Picture: Neuroplasticity Beyond Depression
While depression has been the primary focus of psilocybin neuroplasticity research, the implications extend far beyond mood disorders.
PTSD: Fear-based disorders involve rigid neural circuits that lock people into trauma responses. Research from Kwan’s lab has shown that psilocybin facilitates fear extinction in mice — the process of unlearning fear responses — through neuroplastic mechanisms. This has obvious implications for PTSD treatment.
Addiction: Substance use disorders are associated with reduced prefrontal cortex function and weakened executive control circuits. By rebuilding connections in these areas, psilocybin could help restore the brain’s ability to regulate impulses and make healthier decisions. Early clinical trials at Johns Hopkins have shown promising results for psilocybin-assisted therapy in treating alcohol and tobacco addiction.
Neurodegenerative Diseases: A groundbreaking pilot study from UCSF tested psilocybin on Parkinson’s disease patients and found improvements not just in mood, but in cognition and motor function. The researchers suggested psilocybin may help the brain repair itself by reducing neuroinflammation and promoting neuroplasticity — the same spine-growing mechanism documented at Yale.
Cognitive Flexibility: Even in healthy individuals, psilocybin’s neuroplastic effects may enhance creative thinking, problem-solving, and the ability to break out of rigid thought patterns. This is likely part of why microdosing has become so popular among creatives and professionals.
What This Means for You
If you’re reading this and thinking, “Okay, so psilocybin literally grows new brain connections. What do I do with that information?” — here are some practical takeaways:
1. The Trip Is Part of the Medicine
The 2025 Cell study confirmed that psilocybin’s rewiring is activity-dependent. The neural activity during your experience shapes which connections are built. This means set and setting aren’t just nice-to-haves — they’re biologically important. Go in with intention. Create a safe, comfortable environment. The quality of your experience directly influences the quality of your brain’s restructuring. Our 10 Best Activities on Magic Mushrooms blog can help you plan.
2. Integration Matters More Than You Think
New spines take about 4 days to mature into functional synapses. The weeks following a psilocybin experience are a critical window where your brain is consolidating new connections. This is why integration — journaling, therapy, reflection, and mindful lifestyle choices — is so important. You’re not just processing the experience emotionally; you’re supporting the biological maturation of new neural pathways.
3. Spacing Your Sessions Is Smart Biology
Your brain needs time to build and stabilize new connections. Rushing back for another trip before the previous round of neuroplasticity has matured is counterproductive. The standard recommendation of waiting at least 14 days between sessions isn’t just about tolerance — it’s about giving your brain time to finish its construction project. For more on this, read our full guide on Psilocybin Tolerance.
4. Support Your Brain’s Building Materials
Neuroplasticity requires raw materials: protein, omega-3 fatty acids, B vitamins, adequate sleep, and regular exercise. If you’re interested in maximizing the neuroplastic potential of psilocybin, support your brain with good nutrition, quality rest, and physical activity before and after your experience. Think of it like providing building materials for a construction crew that’s about to get to work.
5. Choose Your Strain Wisely
Different strains produce different intensities of experience, which likely correlates with different levels of receptor activation and neuroplastic stimulation. If you’re specifically interested in the therapeutic and neuroplastic potential, a moderate-to-strong experience with a well-characterized strain is likely more effective than a barely-perceptible microdose. Our guide on How Different Strains Affect Your Experience can help you choose.
Frequently Asked Questions
Does psilocybin actually grow new brain cells?
The Yale research focused on dendritic spines — new connections between existing neurons — rather than entirely new brain cells (neurogenesis). However, other studies have shown that psilocybin can promote neurogenesis in the hippocampus (the growth of brand new neurons), particularly at low to moderate doses. So the answer is: it does both — grows new connections and potentially new cells.
How long do the new connections last?
The Yale study tracked spines for 34 days and found that a significant portion of the new connections were still present. The 2025 Cell study confirmed that the network-level rewiring is also persistent. The exact upper limit isn’t known, but the structural changes appear to last at least several weeks to months.
Do I need a “heroic dose” for neuroplasticity?
Not necessarily. The Yale mouse study used a dose equivalent to a moderate human experience. The neuroplastic effects appear to be dose-dependent, meaning more intense experiences may produce more structural change. But even moderate doses produced significant spine growth. The key is having a meaningful experience, not an overwhelming one.
Can I see these changes on a brain scan?
A 2024 study published in Nature used precision functional mapping (fMRI) in humans and confirmed that a single dose of psilocybin produces detectable changes in brain connectivity that persist for weeks after the experience. So while we can’t see individual dendritic spines in living humans, we can see the larger-scale connectivity changes that result from them.
Is this why psilocybin helps with depression when SSRIs don’t?
Possibly. SSRIs work by increasing serotonin availability but don’t directly promote spine growth. Psilocybin activates the same receptor system but through a different mechanism — an acute burst of 5-HT2A activation that triggers structural remodeling. For people with treatment-resistant depression, this structural approach may address the root cause (lost connections) rather than just managing the symptoms.
The Bottom Line
The science is clear and getting clearer every year: psilocybin doesn’t just change how you feel during a trip. It physically changes the structure of your brain — growing new connections, strengthening communication between neurons, and selectively rewiring neural networks in ways that break the patterns underlying depression, anxiety, and rigid thinking.
From the landmark 2021 Yale study showing a 10% increase in dendritic spine density from a single dose, to the 2025 Cell paper mapping exactly how psilocybin rewires entire brain networks, the evidence paints a consistent picture: this compound promotes rapid, lasting structural change in the brain regions most affected by mental illness.
We’re still in the early chapters of understanding psilocybin’s full neuroplastic potential. But what we know so far is extraordinary — and it explains why so many people describe their mushroom experiences as genuinely life-changing.
Because at a biological level, they are.
Happy tripping!
Curious to explore the neuroplastic potential of psilocybin for yourself? Browse our full selection of magic mushrooms, or start with our microdose capsules for a gentler introduction.
Sources
Shao et al. (2021) — “Psilocybin induces rapid and persistent growth of dendritic spines in frontal cortex in vivo” — Neuron — https://pubmed.ncbi.nlm.nih.gov/34228959/